Introduction
Liver transplantation (LT) is a surgical procedure indicated for patients with end-stage liver disease or acute liver failure that cannot be treated with medication or other therapies. High intraoperative blood loss is anticipated during LT owing to coagulopathy, portal hypertension, collateral vessels, and complex surgical procedures including anastomosis of major vessels [1]. Therefore, allogeneic blood transfusion is common, and rates of perioperative allogeneic blood transfusion remain elevated in patients undergoing LT (50.5%–62.6%) [2,3]. However, allogeneic blood transfusion causes immunosuppression [4] and can lead to complications, such as anaphylaxis, transfusion-associated circulatory overload, or transfusion-related acute lung injury [5,6]. The risk of infection and graft failure is also high in patients who receive allogeneic blood transfusion, with significantly longer wound healing and hospitalization periods [7,8].
In an effort to reduce the need for allogeneic blood transfusions, intraoperative blood salvage autotransfusion (IBSA) has been developed. Moreover, the IBSA system collects and processes blood from the operative field, allowing it to be reinfused into the patient [9].
Studies have reported that IBSA reduces the amount of intraoperative allogeneic red blood cell (RBC) transfusion in LT [10,11]; however, some studies have suggested otherwise [12,13]. Additionally, several reports revealed that higher intraoperative blood loss may be owing to IBSA-related fibrinolysis during LT [14,15]. The relationship between IBSA and the coagulative and fibrinolytic laboratory parameters has not been studied in detail. Moreover, some reports have shown that IBSA can cause side effects, such as coagulopathy, infection, and salvaged blood syndrome [6,16].
Currently there is no consensus on the efficacy and safety of IBSA in LT, and the impact of IBSA on the early and long-term outcomes is unclear. Therefore, this study aimed to evaluate the efficacy of IBSA during LT, with the goal of providing insight into its potential role in reducing the need for allogeneic blood transfusions and improving patient outcomes. Additionally, we verified the efficacy of blood salvage throughout the perioperative period of LT by showing the reduced amount of postoperative allogeneic blood transfusion.
Materials and Methods
This study has been approved by the Institutional Review Board (IRB) of Severance Hospital (IRB No. 4-2022-1629). The requirement for informed consent was waived by the IRB owing to the retrospective nature of this study.
This was a single-center, retrospective cohort study. Data were collected from electronic medical records. Patients who underwent LT between January 1, 2019, and December 31, 2022, were enrolled. The exclusion criteria were ages below 18 years, emergency surgery, deceased donor LT, and incomplete data. Incomplete data refers to data omissions, inadequately recorded information, or data presented in inappropriate formats. Patients undergoing elective living-donor LT were divided into two groups based on usage of IBSA: Cell Saver (CS) group and non-CS group.
Patient demographics (sex, age, height, weight, body mass index, and the model for end-stage liver disease [MELD]), symptoms related with end-stage liver disease (ascites, encephalopathy, and varices), preoperative laboratory findings, perioperative outcomes, and transplantation-related complications were recorded. The MELD score was calculated using the preoperative values for international normalized ratio (INR), serum bilirubin, and serum creatinine. Aspartate transaminase, alanine transaminase, total bilirubin, direct bilirubin, prothrombin time (PT), INR, activated partial thromboplastin time (aPTT), hemoglobin, and platelet count were involved in preoperative laboratory findings within one month prior to surgery. Intraoperative parameters include the amount of crystalloid, albumin input, RBC count, fresh frozen plasma (FFP), platelet count, cryoprecipitate transfusion, urine output, and estimated blood loss. Hemoglobin level, platelet count, PT, INR, aPTT, and fibrinogen were recorded on postoperative day 1 (POD1) and on discharge. Postoperative transfusion was calculated as the total amount of transfused blood from admission to the surgical intensive care until discharge. Clinical outcomes including length of hospital, intensive care unit (ICU) stay and ventilation duration were recorded. We examined transplantation-related complications (graft failure, bile duct complication, and vascular complication) using follow-up data. Patients who underwent surgery between January 1, 2019, and December 31, 2021, were included and followed up until June 2022. The follow-up period ranged from 80 to 1,234 days, with a median of 501 days. These variables were compared between the CS group and non-CS group.
According to our institutional policy, IBSA was used in the elective living-donor LT, whereas it was contraindicated in patients with advanced hepatocellular carcinoma. Blood was salvaged using Cell Saver 5 (Haemonetics®). The shed blood from the operative field was suctioned into the reservoir of a device containing anticoagulant. If sufficient blood was collected, it underwent centrifugation and washing, and was processed to a hematocrit of approximately 60%. The target blood hemoglobin concentration was 8.0 g/dl, and salvaged blood was autotransfused in the CS group when RBC transfusion was indicated. Salvaged blood was used only during surgery.
Intra- and postoperatively, allogeneic blood transfusion was performed based on the hospital guidelines. Allogeneic transfusion was considered based on tolerance when the hemoglobin concentration dropped below 8.0 g/dl that was determined by arterial blood gas analysis or complete blood count.
Statistical analysis
Continuous variables are presented as median (Q1, Q3) or mean ± SD and were compared using a Mann-Whitney U test or independent t-test. Categorical variables are presented as frequency and proportions and were compared using Fisher’s exact test or a chi-square test. The cumulative survival probabilities were estimated by the Kaplan-Meier method and compared between the groups by the log-rank test.
Propensity score matching was performed to correct baseline selection bias. Using logistic regression, a propensity score was constructed based on the predicted probability of IBSA. Selected covariates are variables associated with the degree of liver dysfunction and blood loss during LT. These include sex, age, MELD score, American Society of Anesthesiologists classification, preoperative hemoglobin, platelet count, PT, and INR [17–19]. Covariate matching was performed in a 1:2 ratio between the CS group and non-CS group using an optimal matching algorithm without replacement and caliper. Matching quality was evaluated using standardized mean differences between the CS group and non-CS group. A standardized mean difference < 0.1 indicated a negligible imbalance between the groups.
All two-sided P values < 0.050 were considered statistically significant. Statistical analysis was performed using R package, version 4.2.2 (R Development Core Team, R Foundation for Statistical Computing®). Propensity score matching was performed using the Matchit package of the R software.
Results
A total of 455 LT procedures were performed between January 1, 2019, and December 31, 2022, in our institution. We excluded 100 patients for the following reasons: (1) emergency operation or deceased donor LT (n = 74) and (2) ages under 18 years (n = 26). The remaining 355 adult patients who underwent elective living-donor LT were included in this study.
Of these, 59 (16.6%) received IBSA and 296 (83.4%) did not. Baseline characteristics are shown in Table 1. Before matching, significant differences were observed between the two groups, including MELD score, ascites, encephalopathy, bilirubin, PT, INR, aPTT, and hemoglobin. The MELD score was significantly higher in the CS group than in the non-CS group (10.6 [7.7, 15.7] vs. 15.8 [12.9, 21.6], P < 0.001), indicating an imbalance in baseline liver function between the two groups.
Propensity score matching between the two groups was performed in a 1:2 ratio. After matching, the CS group and non-CS group were in balance for baseline characteristics including MELD score (16.0 [11.3, 21.5] vs. 15.8 [12.9, 21.6], P = 0.437, Table 1).
Follow-up data were collected from 127 patients in the study population to evaluate transplantation-related complications (graft failure, bile duct complication, and vascular complication). Among these patients, after propensity score matching, those who underwent surgery until the year 2021 were included and followed up until June 2022.
The median blood volume autotransfused in the CS group was 550 ml (314, 1,186). No significant difference in crystalloid and albumin input was observed between the two groups. The median amount of transfused allogeneic RBC was significantly lower in the CS group (1,506.0 ml [896.5, 2,170.5] for the CS group vs. 1,957.5 ml [900.0, 3,294.0] for the non-CS group, P = 0.026). No significant difference in the total amount of transfused FFP, platelets, and cryoprecipitate was observed between the two groups. Estimated blood loss during surgery was not significantly different between the groups (P = 0.611, Table 2).
Both groups showed similar postoperative laboratory findings on POD1 and at the time of discharge (Table 3). The total amount of postoperative RBC transfusion until discharge was significantly lower in the CS group than in the non-CS group (1,500.0 ml [300.0, 3,600.0] vs. 2,100.0 ml [600.0, 4,800.0], P = 0.039). No significant difference was observed between the groups regarding the total amount of postoperative FFP, platelet, and cryoprecipitate transfusion until discharge. The length of hospital and ICU stay and ventilation duration were similar between the groups. Additionally, no significant difference in transplantation-related complications was observed between the two groups, including graft failure, bile duct complication, vascular complication, and one-year mortality (Table 4).
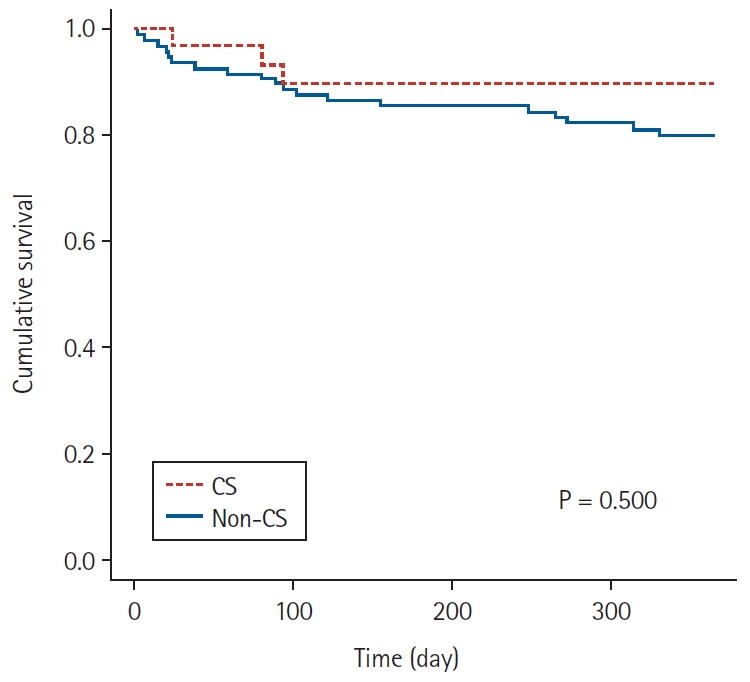
The one-year survival after LT between the CS group and non-CS group was analyzed. The one-year mortality rate was 10% in the CS group, compared to 19.6% in the non-CS group (P = 0.349, Table 4). No significant difference in cumulative survival probabilities was observed between the two groups (P = 0.500, Fig. 1).
Discussion
Our study has demonstrated that IBSA effectively reduces the need for allogeneic blood transfusion during LT throughout the postoperative period until discharge. Moreover, no significant differences in length of hospital and ICU stay, ventilation duration, one-year mortality, and transplantation-related complications were observed between the groups.
The efficacy and safety of IBSA use has been well-established in other surgical domains. A previous systematic review demonstrated that IBSA lowered intraoperative allogeneic RBC transfusion by 38% in orthopedic and cardiac surgery without additional worsening of clinical outcomes [20]. A meta-analysis that included various types of surgery, predominantly consisting of orthopedic, cardiac, and vascular surgeries, demonstrated that IBSA reduced the rate of exposure to allogeneic RBC transfusion by a relative 39%, as well as the risk of infection and length of hospital stay [21]. Compared to research on IBSA in other surgical fields, studies on IBSA in LT are relatively scarce in terms of quantity and sample size. The use of IBSA in LT has been analyzed in several observational studies. Similar to the results of our study, a reduction in intraoperative allogeneic transfusion owing to IBSA use was reported by several studies [22–24].
In addition to the significant reduction in intraoperative RBC transfusion, our study found a noteworthy decrease in postoperative RBC transfusion from the patients’ arrival in the ICU until discharge. This finding is clearly different from that of previous studies that primarily focused on the amount of blood transfused solely during the surgery. However, it aligns with some existing literature [24,25] and suggests a potential correlation with the adverse effects of intraoperative allogeneic transfusion that can cause dilutional coagulopathy and subsequent increase in postoperative bleeding [11]. Based on these observations, it can be speculated that IBSA may enhance postoperative outcomes by reducing the need for intraoperative RBC transfusions without introducing any additional side effects. Although our study did not directly measure postoperative estimated blood loss in the ICU, our results indicated that IBSA did not cause postoperative coagulopathy. These findings suggest that IBSA can be a valuable approach in LT, as it not only reduces the risks associated with allogeneic blood transfusions but contributes to improved postoperative outcomes without compromising coagulation.
Monitoring perioperative blood coagulation in LT is crucial as patients with end-stage liver disease often experience impaired coagulation. In our study, no significant differences were observed intraoperatively between the two groups regarding the transfusion of FFP, platelets, and cryoprecipitate. Furthermore, no notable variations in postoperative laboratory parameters, including platelet count, PT, INR, aPTT, and fibrinogen levels, on POD 1 were observed between the two groups. Since IBSA replaces only RBCs and no other clotting factors or platelets, there is a concern that dilution of clotting factors could potentially lead to clinical coagulopathy [9,26]. However, it is essential to note that several studies have reported that IBSA does not significantly affect the total amount of intraoperative FFP and platelet transfusions, nor does it have a notable impact on postoperative coagulation parameters [20,27]. Additionally, a previous study reported that the volume of IBSA used was associated with the severity of blood coagulation impairment [28]. In studies where clinical coagulopathy was reported, the volume of IBSA used was approximately 1,000 ml that was larger than that used in other studies [28,29]. However, in our study, the average autotransfusion volume was 550 ml that indicates that the volume did not significantly affect blood coagulation. Therefore, based on the findings from our study and existing literature [20,27], it can be suggested that a mean IBSA autotransfusion volume of 550 ml in LT, as used in our research, is unlikely to have a significant effect on blood coagulation. Nevertheless, continuous monitoring and further investigation of perioperative coagulation status remain essential to ensure patient safety during the LT procedures.
This study offers a distinctive and valuable contribution to the existing literature by exploring the cumulative perioperative transfusion volume until discharge. Unlike previous studies that focused solely on the intraoperative outcome, our approach provides a more comprehensive and thorough evaluation of the efficacy of blood salvage throughout the perioperative period of LT. This broader perspective allows for a better understanding of the overall impact and benefits of blood salvage techniques in LT, making our study a valuable addition to the existing body of knowledge in this field.
This study has some limitations. First, being a retrospective study, there may be inherent biases and limitations associated with the use of electronic medical records for data collection, such as potential confounding variables and missing data, and the effect of anesthesiologists or operating surgeons. However, we made efforts to address these limitations by conducting rigorous data collection and employing propensity score matching. Propensity score matching allowed us to minimize selection bias and enhance the comparability between the CS and non-CS groups. Second, the study was conducted at a single center that may restrict the generalizability of our findings to other institutions. To validate and strengthen our results, multi-center studies with larger sample sizes are warranted. Furthermore, the follow-up period in our study was relatively short, ranging from 80 to 1,234 days, with a median of 501 days. Longer-term follow-up is essential to assess the effect of IBSA on outcomes such as overall survival, graft survival, and long-term complications. Future research should focus on evaluating the longer-term effects of IBSA on patient outcomes to gain a more comprehensive understanding of its benefits.
In conclusion, our study presents compelling evidence that the implementation of IBSA during LT is highly effective in reducing the necessity for allogeneic blood transfusions. Our findings hold crucial implications for clinical practice, as IBSA has the potential to substantially decrease the reliance on allogeneic blood transfusions, thereby minimizing transfusion-related complications and ultimately leading to improved patient outcomes. Continued investigation into IBSA’s benefits and appropriate indications could bring about meaningful advancements in the field of LT and enhance patient care in the future.