Introduction
It is crucial to determine the appropriate timing of surgery in patients with preoperative coronavirus disease 2019 (COVID-19) infection. COVID-19 infection is associated with multiple organ injuries [1,2] that may have unexpectedly extended aftereffects [3]. Preoperative COVID-19 infection is associated with increased postoperative morbidity and mortality [4]; however, postponing the surgery can also worsen postoperative outcomes and increase medical costs [5,6], especially in cancer surgeries [7]. This further demonstrates why it is vital for anesthesiologists to determine the appropriate surgery timing for patients with a history of COVID-19 infection before surgery.
An international prospective cohort study published in 2021 reported that preoperative COVID-19 infection within seven weeks before surgery was associated with an increase in postoperative 30-day mortality [8]. Consequently, recommendations from the expert consensus for managing surgical patients with a history of COVID-19 infection have been established in several countries based on this result [9–12], with other studies reporting consistent findings [13,14]. However, the patients in this international prospective cohort study were recruited in October 2020 [8] before the introduction of COVID-19 vaccines, and the severity of COVID-19 infection was worse than it is now [15]. COVID-19 vaccination in South Korea started in February 2021. There is a need for a more comprehensive investigation of the influence of preoperative COVID-19 infection on surgical prognosis due to the increased availability of vaccines and medical resources since the initial outbreaks [16–18].
Therefore, in this retrospective study, we aimed to examine the association between preoperative COVID-19 infection and 30-day postoperative mortality in patients who underwent surgery in 2021 using the Korea Disease Control and Prevention Agency–COVID-19 National Health Insurance Service (K-COV-N) cohort data. Our results could help determine the appropriate timing of surgery during the vaccination era in patients with a history of COVID-19 infection.
Materials and Methods
Study design and population
This nationwide retrospective cohort study’s protocol was exempted from review by our institution’s Institutional Review Board due to the study’s retrospective nature and the use of de-identified data. This study was also approved by the Korea Disease Control and Prevention Agency (KDCA) and National Health Insurance Service (NHIS) (approval number: KDCA-NHIS-2022-1-620). The present study was also conducted following the principles outlined in the Declaration of Helsinki, 2013 and has been reported following the STrengthening the Reporting of OBservational studies in Epidemiology guidelines [19].
Notably, all data were obtained from the K-COV-N cohort database combined with the KDCA and NHIS data. Korea has a universal compulsory national health insurance system that covers virtually all Korean residents [20]. The NHIS database contains information regarding all inpatient and outpatient medical services, including diagnoses based on the International Classification of Diseases 10th Revision (ICD-10) codes, prescription, and prescription codes. In addition, the KDCA database contains detailed information regarding COVID-19 confirmation and vaccination. Therefore, the K-COV-N cohort database includes data regarding the confirmation date of COVID-19 infection and the data on the date and type of the COVID-19 vaccination.
We included patients who underwent surgery under general anesthesia (procedure codes: L0101, L1211, and L1212) in South Korea between January 2021 and December 2021. The K-COV-N cohort database provided information regarding the COVID-19 confirmation date between October 8, 2020, and December 31, 2021. Notably, only the confirmation year was obtained for patients before this period. We excluded patients who did not undergo predefined standard surgery during the study period. Standard surgery was defined based on a list of procedure codes used to establish surgical healthcare statistics that inform national health policies in Korea. The procedure codes were listed in the NHIS’s Main Surgery Statistical Yearbook for 2020 and the Standard Guide to Statistics of Disease and Procedure published by the Health Insurance Review and Assessment Service in Korea (Supplementary Table 1) [21,22]. Moreover, we excluded patients diagnosed with COVID-19 within 30 days after the index surgery. Only the first surgery was analyzed if a patient underwent multiple standard surgeries.
Data collection
We collected data regarding demographics (age and sex), preoperative comorbidity (congestive heart failure, dementia, chronic pulmonary disease, rheumatologic disease, mild liver disease, diabetes with chronic complications, hemiplegia or paraplegia, renal disease, any malignancy, including leukemia and lymphoma, moderate or severe liver disease, metastatic solid tumor, acquired immune deficiency syndrome, or human immunodeficiency virus infection), confirmation date of COVID-19 infection, COVID-19 vaccination-related variables (vaccination date, vaccination series, and vaccine type), surgery-related variables (department of surgery, surgical type, relative work unit, and urgency), income level (as quartiles), residence level (capital city, metropolitan city, or other areas), postoperative complications within 30 d after surgery, and date of all-cause death. Preoperative comorbidities were indicated by at least two corresponding ICD-10 codes recorded within one year before surgery (Supplementary Table 2). The updated Charlson comorbidity index (CCI) score was also calculated [23]. The status of COVID-19 vaccination was considered ‘fully vaccinated’ if patients received at least one dose of Ad.26.COV2.S or at least two doses of BNT162b2 or mRNA-173 vaccines 14 d before the index surgery [24]. ‘Not fully vaccinated’ was defined as receiving only one BNT162b2 or mRNA-173 vaccine 14 days before the surgery; otherwise, patients were regarded as ‘not vaccinated.’ We did not consider the period between vaccination and COVID-19 confirmation due to a previous report on the beneficial effect of COVID-19 vaccination in patients without COVID-19 infection [16]. The guidelines for COVID-19 vaccination in South Korea recommend vaccination at least four weeks after COVID-19 confirmation [25]. The relative work unit is a calculated score that considers the relative risk of medical practice in South Korea, and it was used to classify the risk of surgery into quartiles (first quartile, very low-risk surgery; second quartile, low-risk surgery; third quartile, intermediate-risk surgery; fourth quartile, high-risk surgery). Postoperative complications within 30 days after surgery were derived from the NHIS database using the corresponding ICD-10 diagnostic codes. Supplementary Table 3 summarizes the ICD-10 codes for postoperative complications [26].
Study group and outcomes
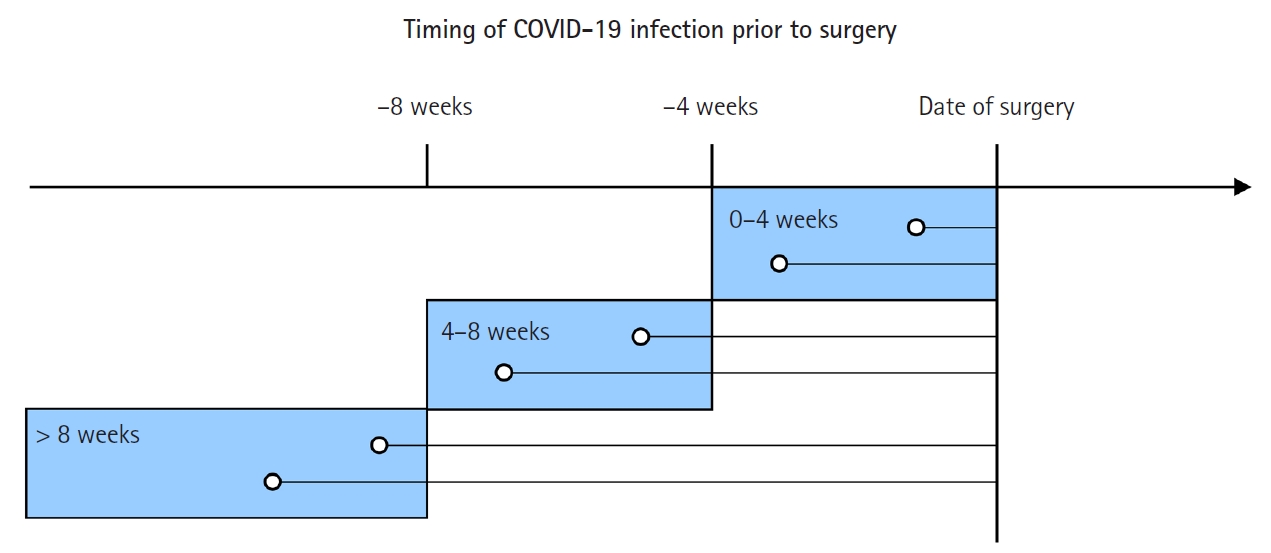
Patients were categorized into four groups based on the duration from the confirmation date of COVID-19 infection to the date of index surgery [24,27]: 0–4 weeks, 5–8 weeks, > 8 weeks, and those without a preoperative history of COVID-19 (Fig. 1). During the study period, a COVID-19 real-time reverse transcription polymerase chain reaction test confirmed COVID-19 infection following the nationwide Korean policy [28]. This study’s primary outcome was the 30-day postoperative mortality. The secondary outcomes were 90-day postoperative mortality and 30-day respiratory complications.
Statistical analyses
All statistical analyses were performed using SAS® version 9.4 (SAS Institute). Statistical significance was set at a two-sided P value < 0.05. Continuous variables are appropriately reported as the mean (standard deviation) or median (interquartile range), whereas categorical variables are reported as numbers (percentage).
We performed among-group comparisons of the 30-day postoperative mortality using logistic regression analyses. Firth correction was used to mitigate bias associated with rare events [29]. Univariate logistic regression analyses for the primary outcome were performed for the study group with the following potential confounders: age, female sex, CCI score, COVID-19 vaccination status, emergency surgery (vs. elective surgery), risk of surgery (as quartiles), income level (as quartiles), and residence level. Age (0–49 years, 50–69 years, and ≥ 70 years) and CCI score (0–3, 4–5, and ≥ 6) were considered categorical variables. The COVID-19 vaccination status was dichotomized into a binary variable (fully vaccinated vs. not or not fully vaccinated). After the univariate analyses, the study group and other confounders were entered into multivariable analysis without the variable selection method. The absence of multicollinearity among variables was confirmed by examining the variance inflation factor (< 2) before incorporating the variables into the multivariable model. The results are reported as odds ratios (ORs) with 95% CIs. In addition, we calculated the C-statistic of the multivariable model. Logistic regression analyses were repeated for the secondary outcomes using methods similar to that for the primary outcome.
Subgroup analyses of the primary outcome were performed to investigate whether the effect of preoperative COVID-19 infection differed according to subgroups. Multivariable logistic regression analyses with adjustment for all these confounders were performed in each subgroup: age (0–49 years, 50–69 years, and ≥ 70 years), sex, CCI score (0–3, 4–5, and ≥ 6), COVID-19 vaccination status, risk of surgery, income level, and residence level. The P-value for interaction was estimated using a likelihood ratio test, wherein multivariable models with and without the interaction term were compared.
Results
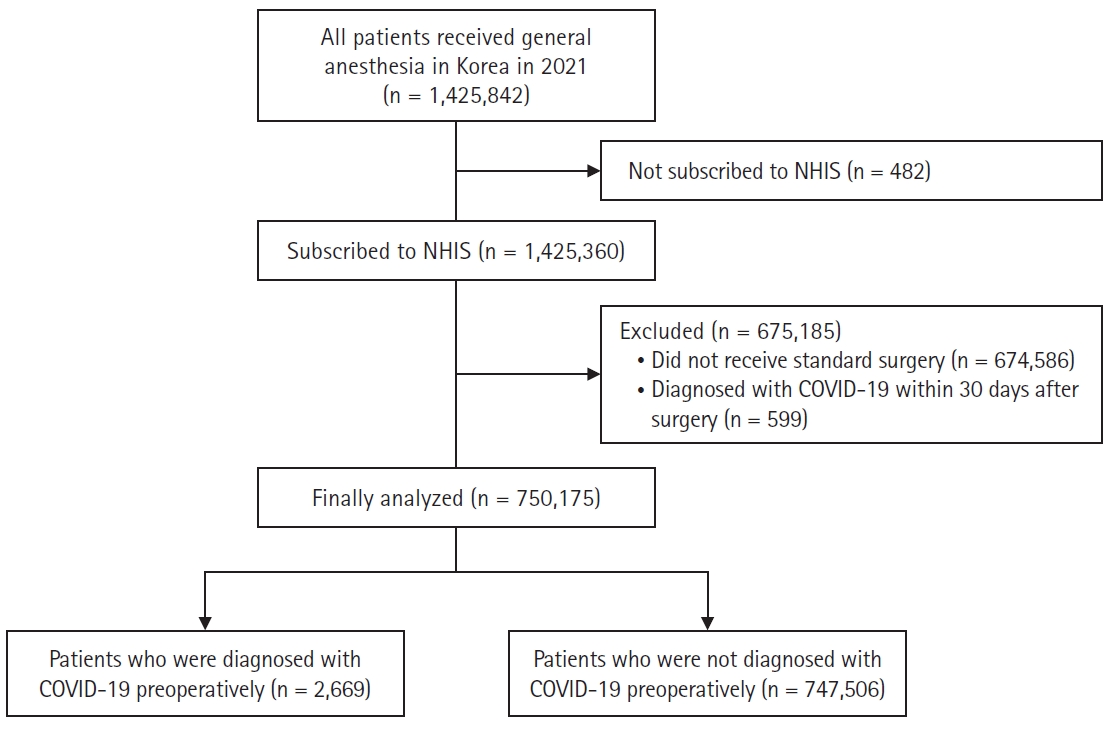
In total, 1,425,360 patients received general anesthesia in South Korea in 2021. After excluding patients who did not undergo predefined standard surgery (n = 674,586) and those who were diagnosed with COVID-19 within 30 days after surgery (n = 599), the remaining 750,175 patients were included in the final analysis (Fig. 2). Among them, 2,669 (0.36%) patients were diagnosed with COVID-19 infection before the surgery. Regarding the duration from the confirmation date of COVID-19 infection to the index surgery date, 352 (0.05%), 474 (0.06%), and 1,843 (0.25%) patients underwent surgery at 0–4 weeks, 5–8 weeks, and > 8 weeks after COVID-19 infection, respectively. The baseline characteristics and surgical variables are summarized in Supplementary Table 4. Among the analyzed patients, 28.2% were identified as fully vaccinated before surgery.
The postoperative outcomes are summarized in Table 1. The incidence rates of 30-day postoperative mortality were 0.4% (3,331/747,506) in patients without prior COVID-19 infection and 1.4% (5/352), 1.3% (6/474), and 0.5% (10/1,843) in patients who underwent surgery at 0–4 weeks, 5–8 weeks, and > 8 weeks after COVID-19 infection, respectively.
The univariate and multivariable logistic regression analysis results for 30-day postoperative mortality are presented in Table 2 and Supplementary Table 5. Compared with patients without prior COVID-19 infection, those who underwent surgery at 0–4 weeks (adjusted OR: 4.28, 95% CI [1.81, 10.13], P = 0.001) and 5–8 weeks (adjusted OR: 3.38, 95% CI [1.54, 7.44], P = 0.002) after COVID-19 infection were significantly associated with a higher risk of 30-day postoperative mortality, respectively. However, there was no significant association between patients who underwent surgery more than eight weeks after COVID-19 infection and risk of 30-day mortality compared with those without prior COVID-19 infection (adjusted OR: 1.58, 95% CI [0.85, 2.92], P = 0.146). In addition, higher age, male sex, higher CCI score, emergent surgery, higher risk of surgery, lower income level, and residence, except for the capital city, were associated with a higher risk of 30-day postoperative mortality. However, a fully vaccinated status (OR: 1.00, 95% CI [0.93, 1.07], P = 0.916) was not associated with a significantly lower risk of 30-day postoperative mortality. The C-statistic of the multivariable model for predicting 30-day postoperative mortality was 0.823.
Multivariable logistic regression analysis of 90-day mortality is presented in Table 2 and Supplementary Table 6. Patients who underwent surgery at 0–4 weeks (adjusted OR: 3.13, 95% CI [1.61, 6.10], P = 0.001) and 5–8 weeks (adjusted OR: 2.34, 95% CI [1.25, 4.38], P = 0.008) after COVID-19 infection were significantly associated with a higher risk for 90-day postoperative mortality than those without prior COVID-19 infection. Patients who underwent surgery more than eight weeks after COVID-19 infection were not significantly associated with 90-day postoperative mortality (P = 0.856). Fully vaccinated status was associated with a substantially lower risk of 90-day postoperative mortality (OR: 0.93, 95% CI [0.89, 0.98], P = 0.007). The C-statistic of the multivariable model for predicting 90-day postoperative mortality was 0.819.
In the multivariable logistic regression analysis, patients who underwent surgery 0–4 weeks after COVID-19 infection were significantly associated with an increased risk of 30-day respiratory complication (adjusted OR: 3.79, 95% CI [2.66, 5.40], P < 0.001) (Supplementary Table 7). However, patients who underwent surgery at 5–8 or > 8 weeks after COVID-19 infection were not significantly associated with 30-day respiratory complications (P = 0.096 and 0.134, respectively). A fully vaccinated status was associated with a substantially lower risk of 30-day respiratory complications (OR: 0.85, 95% CI [0.82, 0.87], P < 0.001). The C-statistic of the multivariable model for predicting 30-day respiratory complications was 0.658.
The subgroup analyses showed no significant interaction effects between preoperative COVID-19 infection and covariates on 30-day postoperative mortality (Supplementary Tables 8 and 9).
Discussion
Our study showed a significant association between COVID-19 infection within eight weeks before surgery and 30-day postoperative mortality, consistent with previous reports [8,13,14,27]. Preoperative COVID-19 vaccination was not significantly associated with a decrease in 30-day postoperative mortality. However, it significantly correlated with reduced 90-day postoperative mortality and 30-day respiratory complications. The subgroup analyses showed no significant interaction effects between preoperative COVID-19 infection and the predefined covariates on 30-day postoperative mortality. This suggests that the association between COVID-19 infection occurring within eight weeks preoperatively and the risk of 30-day postoperative mortality might remain uniform across all the subgroups. Our findings may provide additional meaningful information on this critical issue given that our patient cohort comprised more vaccinated patients and thus reflected a more contemporary community vaccination status compared with previous studies [8,13,30].
We observed a significant association between preoperative COVID-19 infection and 30-day postoperative mortality, inconsistent with a recent report of a nonsignificant association between them [30]. Specifically, this previous study found that preoperative COVID-19 infection, even less than four weeks prior, was not associated with worsened postoperative outcomes following elective major noncardiac surgery [30]. In addition, they observed a nonsignificant association between preoperative COVID-19 vaccination and postoperative outcomes. Notably, the study included a relatively contemporary patient population between April 2020 and October 2021; these nonsignificant results were attributed to the fact that their medical resource was less affected by the COVID-19 pandemic than earlier studies. Moreover, relatively small number of patients with preoperative COVID-19 infection (960 patients), and significantly low rates of death and major adverse cardiovascular events suggest that the study were inadequately powered to find a significant association between preoperative COVID-19 infection and postoperative outcomes.
Our study could not find a significant association between preoperative COVID-19 vaccination and 30-day postoperative mortality; however, it did show a significant association with reduced 90-day postoperative mortality and decreased 30-day respiratory complications. COVID-19 vaccination status can have a significant effect on postoperative outcomes. The availability of the COVID-19 vaccine that was available in the United States and the United Kingdom from December 2020 was a crucial turning point in the COVID-19 pandemic [31,32]. COVID-19 vaccination weakens the severity of COVID-19 infection, reducing COVID-19 infection-related hospitalizations and deaths [33,34]. These positive effects of COVID-19 vaccination have also been reported in surgical patients. A recent nationwide retrospective study reported that preoperative COVID-19 vaccination significantly reduced postoperative pulmonary complications and the length of hospital stay at Veterans Affairs facilities [16]. However, there was no significant association between preoperative COVID-19 vaccination and postoperative mortality due to the minimal number of events [16]. Conversely, their subsequent larger-scale study observed a significant association of preoperative COVID-19 vaccination with a decrease in postoperative mortality, regardless of the degree of preoperative vaccination [35]. In contrast, our study failed to demonstrate a significant association between preoperative COVID-19 vaccination and 30-day postoperative mortality. The postoperative 30-day period may not have sufficiently observed the benefits of preoperative COVID-19 vaccination. Although 30-day postoperative mortality is one of the widely used indicators of postoperative outcomes, there have been arguments that it is less effective in reflecting perioperative outcomes compared to 90-day postoperative mortality [36,37]. Moreover, although our study included a large sample size of 750,175 individuals, the 30-day postoperative mortality rate was only 0.4%. In addition, the initial phase of vaccination in South Korea that primarily targeted individuals with underlying health conditions or those in older age groups following the government’s priority policy may also have influenced these results [38]. Nevertheless, since preoperative COVID-19 vaccination showed a significant association with a decrease in 90-day postoperative mortality and 30-day respiratory complications, further research is required to determine the effect of preoperative COVID-19 vaccination on postoperative outcomes.
Notably, we could not confirm whether full vaccination can completely offset the impact of preoperative COVID-19 infection on postoperative mortality [24]. A previous large-scale retrospective study reported that preoperative COVID-19 infection was not significantly associated with postoperative complications at any time interval in fully vaccinated patients; however, preoperative COVID-19 infection within four weeks was significantly associated with increased postoperative complications in patients who were not fully vaccinated [24]. Another retrospective study reported that the time interval from preoperative COVID-19 infection to surgery was negatively associated with the rate of major cardiovascular postoperative complications, even in patients who had received at least one dose of the COVID-19 vaccine preoperatively [39]. Furthermore, since the COVID-19 vaccine against the Omicron variant is less effective than that against the Delta variant and the effectiveness wanes over time [33,40,41], it is difficult to disregard the effect of preoperative COVID-19 infection, even in fully vaccinated patients. Therefore, further studies are required to explore the association between the status of COVID-19 vaccination and postoperative outcomes in more contemporary patient populations.
This study has some limitations. First, despite the robust adjustments undertaken in the analysis, there may be residual confounding factors due to the inherent limitations of a retrospective study design. Precisely, we could not determine whether patients with preoperative COVID-19 infection had COVID-19-related symptoms at the time of the index surgery. Current guidelines recommend that patients with a history of COVID-19 infection are scheduled for elective surgery seven weeks after the infection. In addition, the decision to proceed or delay the surgery should be made based on the presence or severity of persistent COVID-19 symptoms [9]. Second, our study involved patients who underwent index surgery before the emergence and predominance of the Omicron variant of COVID-19. Since the Omicron variant is less likely to cause severe infections compared with the Delta variant [33,42], our results may not be directly generalizable to patients infected with the Omicron variant. Third, we could not analyze the effect of administering booster vaccine doses. In Korea, booster doses became available nationwide in October 2021, and the proportion of patients who received the booster dose before the index surgery was significantly small. Further studies are necessary to clarify this issue. Fourth, given our cohort’s remarkably low mortality rate, we set the between-group interval as four weeks rather than two weeks to ensure an adequate mortality incidence for statistical analysis in each group. Finally, the 30-day mortality rate was 0.4%, significantly lower than previously reported values [8]. Since there is a considerable disparity in postoperative mortality rates among different countries [43], it may be inappropriate to directly extrapolate our findings to patients in other countries.
In conclusion, our study found a significant association between COVID-19 infection within eight weeks preoperatively and an increased risk of 30-day postoperative mortality, regardless of the preoperative vaccination status. Our study suggests that anesthesiologists should carefully determine the timing of surgery for patients who have a recent history of COVID-19 infection but are yet to receive COVID-19 vaccination. Further studies will also be required to reflect the current status of COVID-19 infection on this issue.