Introduction
Adequate postoperative pain control can improve postoperative recovery and reduce morbidity.
Several adjuvants have been used to enhance analgesia and prolong the analgesic duration, as well as reduce opioid requirements and related side effects.
Corticosteroids have a powerful anti-inflammatory action and have demonstrated reduced pain and swelling after various surgeries, but the exact mechanism of the analgesic effect is not fully understood [1,2]. Steroids are also known to inhibit phospholipase A2 and the expression of cyclooxygenase-2 during inflammation. Thus, reduced prostaglandin synthesis suppresses hyperalgesia associated with acute nociception during surgery [3]. Although steroids given epidurally were effective in the treatment of lower back pain [4], in addition to reducing postoperative pain and analgesic requirements [5], the potential efficacy of postoperative analgesia has not been elucidated.
This study was designed to investigate whether postoperative pain could be alleviated by epidural administration of dexamethasone in patients undergoing major abdominal surgery.
Materials and Methods
This randomized controlled study was approved by the institutional review board and written informed consent was obtained from all study participants. Ninety patients (age 30-77 and having American Society of Anesthesiologists physical status I and II) scheduled for radical subtotal gastrectomy due to stomach cancer by a single surgeon were included to this study from June 2009 to July 2010. Patients with a history of cardiac, respiratory, neuromuscular, hepatic or major renal disease were excluded from this study. Patients were also excluded if they were obese, diabetic, had local infection, spinal anomalies, infectious diseases, neurologic disorders, seizures and coagulopathies or if they were receiving analgesics, corticosteroids or calcium channel blocking drugs.
Using computer generated randomization, patients were allocated to three groups: Group I (n = 30, local anesthetics only), Group II (n = 30, epidural dexamethasone, 5 mg prior to surgery), and Group III (n = 30, epidural dexamethasone, 5 mg at the end of surgery). The patient and the investigator involved in the data collection were not aware of the patient group assignment/treatment. All drugs used for epidural injection (0.25% ropivacaine with 5 mg dexamethasone or same volume of saline) were prepared in the anesthesia preparation room by a nurse who was blinded to the study. Anesthetic practitioners, who were also blinded to the group allocation, managed the anesthesia.
On arrival to the operating room, standard monitors were applied to the patients. Epidural paramedian puncture was performed at the T7-8 interspace with 17 G Touhy needle in the lateral decubitus position. After identifying the epidural space with loss of resistance technique, a 20 G multi-orifice epidural catheter was threaded and advanced 6 cm cephalad and safely fixed. Successful epidural catheterization was confirmed with sensory changes after a test dose of 2% lidocaine (3 ml) was injected. Anesthesia was induced with propofol and remifentanil infusion. Tracheal intubation was performed after rocuronium administration and anesthesia was maintained with sevoflurane in air/O2 (FiO2 = 0.5). Supplemental remifentanil was continuously infused. In all groups, 10 ml of 0.25% ropivacaine was injected epidurally before the start and at the end of the operation. In Group I, epidural ropivacaine without dexamethasone was epidurally administered. In Group II, epidural dexamethasone (5 mg) was added to the bolus ropivacaine injection before the start of operation. In Group III, the same amount of dexamethasone was given with the epidural ropivacaine treatment at the end of operation.
During surgery, the anesthetic depth was maintained within a range of ± 20% from baseline values for heart rate and arterial blood pressure and the bispectral index was maintained within a range of 40-60. Subtotal gastrectomy with gastroduodenostomy (Billoth I) surgery was then initiated. After the second bolus epidural injection, an infusion device (Automed-3200®, Ace-medical, Seoul, Korea) prefilled with 0.15% ropivacaine and 1,000 µg of fentanyl with a total volume of 250 ml was connected to the epidural catheter. The infusion device was programmed with a basal infusion rate of 5 ml/h without an intermittent bolus dose. After the surgery, the residual neuromuscular blockade was reversed with pyridostigmine and glycopyrrolate, and then 4 mg of ondansetrone was given. When the patient responded to verbal commands and neuromuscular function was ascertained by 4 responses of the adductor pollicis to train of four stimulation with sufficient spontaneous respiration determined by tidal volume and respiratory rates, the tracheal tube was removed. In the post-anesthesia care unit (PACU), postoperative pain was assessed using the visual analog scale (VAS) score at rest and with effort (i.e. coughing and at 30° sitting) at 5 minutes (T1) and 30 minutes (T2) after entry. When the patient requested an analgesic, 50 µg of fentanyl was administered i.v. in the PACU. After discharge from the PACU, two nurse investigators blinded to the study groups assessed the pain scores 24 h (T3) and 48 h (T4) after surgery. The incidence of adverse effects, such as peripheral oxygen desaturation (SpO2 < 90%), nausea or vomiting, somnolence, and pruritus (rubbing or scratching the skin) were recorded. Patients were instructed to request analgesics from the nurse when needed. Meperidine (25 mg, i.v.) was given as the rescue analgesic.
All data were analyzed with PASW Statistics 18® (SPSS Inc., Chicago, IL, USA). Continuous variables were shown as mean ± SD and categorical variables were shown as numbers. A series of one-way ANOVAs were conducted to examine differences among the 3 groups with respect to parametric variables followed by student's t test. Categorical variables were analyzed using the chi-square test or Fisher's exact test, as appropriate. A P value of <0.05 was considered significant.
Results
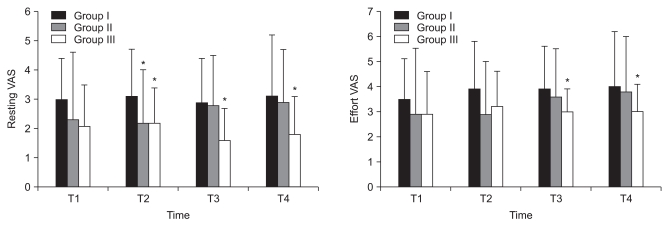
There were no significant differences in patient characteristics between groups (Table 1). The resting VAS was significantly lower in Group II at T2 compared to Group I. In Group III, the resting VAS was significantly lower at T2, T3, and T4 than in Group I. The effort VAS was significantly lower in Group III than in Group I at T3 and T4 (Fig. 1).
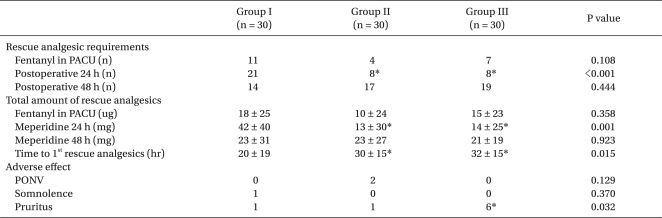
Postoperative rescue analgesic requirements and adverse effects are shown in Table 2. In the PACU, fentanyl was given in 11 patients in Group I, 4 in Group II, and 7 in Group III and there were no significant differences in the total amount of rescue fentanyl (P = 0.358). The total requirements of rescue meperidine were significantly less in Groups II and III as compared to Group I at postoperative 24 h (P = 0.001) but, there were no significant differences at postoperative 48 h (P = 0.923). No significant differences were found in the incidence of nausea and vomiting between the groups. The frequency of pruritus was higher in Group III compared to Groups I and II (Table 2). No one showed peripheral oxygen desaturation (SpO2 < 90%) throughout the study period.
Discussion
In patients undergoing gastrectomy, high thoracic epidural catheterization is commonly performed to provide continuous postoperative pain control. In spite of continuous epidural pain control, some patients frequently request additional analgesics. In our study, rescue analgesics were required in 8.9% of patients within 5 minutes of arrival in the PACU, in 15.6% by 30 minutes, in 41% within 24 h and in 55.6% by postoperative hour 48.
Epidural steroid injection is a common modality for treatment of chronic pain. Dexamethasone has been demonstrated to reduce lumbar epidural puncture-induced backache [4], postoperative pain, and morphine consumption [5]. We conducted this study to assess the effects of epidurally administered dexamethasone on postoperative analgesia after major abdominal surgery. Although the underlying mechanism(s) of epidural steroid and local anesthetics are still not well understood, it is considered that the neural blockade alters or interrupts nociceptive input, reflex mechanisms of the afferent fibers, self-sustaining neuronal activity and the pattern of central neuronal activities [6]. In addition, steroids reduce inflammation by inhibiting either the synthesis or release of a several pro-inflammatory mediators and by causing a reversible local anesthetic effect. Epidural dexamethasone administration has been shown to reduce postoperative analgesic requirements in dental, laparoscopic and breast surgeries [7-10].
However, there have been no studies investigating the effect of epidural dexamethasone treatment on pain after major abdominal surgery. The major finding of this study was that 5 mg of epidurally administered dexamethasone was effective in reducing the degree of pain and rescue analgesic requirements after radical subtotal gastrectomy during the early postoperative period.
Acute noxious stimulation of peripheral tissues leads to sensitization of dorsal horn neurons of the spinal cord by the release of excitatory amino acids such as glutamate and aspartate. These amino acids activate N-methyl-D-aspartate receptors resulting in calcium ion influx. As a result, increased intracellular calcium activates phospholipase A2 which converts membrane phospholipids to arachidonic acid. Simultaneously, there is up-regulation of the expression of cyclo-oxygenase 2 in the spinal cord, leading to prostaglandin E2 synthesis, which results in a hyperalgesic state [1,3]. Epidural dexamethasone administration may influence intraspinal prostaglandin synthesis by inhibiting phospholipase A2 and the expression of cyclo-oxygenase 2 [1]. Steroids also suppress transmission in thin unmyelinated C-fibers and bind directly to the intracellular glucocorticoid receptor [11].
The exact onset time of dexamethasone is unclear and the appropriate timing for administration is still controversial. Some have reported preoperative administration of epidural dexamethasone reduces postoperative pain and analgesic requirements [5,12]. Tissue injured during surgery acts as an acute noxious stimulation to other tissues. Thus, it leads to activation of phospholipase A2 and the expression of cyclooxygenase 2 in the spinal cord, resulting in prostaglandin synthesis and induction of a hyperalgesic state [3]. Preoperative administration of steroids may reduce these reactions and improve analgesia [9]. In a recent meta-analysis, preoperative or postoperative epidural steroid treatment decreased pain and shortened the length of hospital stays after lumbar spinal surgery [13]. In our study, the preoperative dexamethasone group (Group II) had a low resting VAS after 30 min in the PACU and the postoperative dexamethasone group (Group III) had a low resting VAS after 30 min of PACU as well as 24 and 48 h postoperatively. Effort VAS for Group II was also significantly higher than in Group III and there was no difference when compared to Group I.
Because we could not rule out the possible bias in pain assessment, we evaluated the number of rescue analgesic requirements and total amount of rescue opioid used. The time to the first rescue analgesic requirement was longer and the total amount of rescue meperidine used during the first 24 h of the postoperative period was less in the dexamethasone-treated groups (Group II and III) than in the group not receiving dexamethasone (Group I). Although we could not conclude the proper time to administer epidural dexamethasone because pain is very subjective and affected by many factors, epidural dexamethasone administration may alleviate the pain after major abdominal surgery.
The incidence of postoperative nausea and vomiting as well as somnolence was not significantly different between groups. However, the frequency of an itching sensation was higher in Group III. Ironically, i.v. dexamethasone-induced perineal pruritus has been described in patients with chemotherapy and acute head injury in an attempt to reduce intracranial pressure and oral surgery [14-16]. This adverse effect can be prevented by slowly giving diluted dexamethasone [17]. Also, because intrathecally or epidurally administered opioid-induced pruritus is not associated with histamine release, H1 blockers have little effect on the development of pruritus after opioid administration [18,19]. In our study, no one showed perineal pruritus and all symptoms of pruritus were relieved by the administration of diphenhydramine.
In conclusion, the epidural administration of 5 mg of dexamethasone can reduce the pain and rescue analgesic requirements 24 h after radical subtotal gastrectomy. Further study is required for determination of the proper timing of dexamethasone administration.