Ultrasound-guided trans-incisional quadratus lumborum block versus ultrasound-guided caudal analgesia in pediatric open renal surgery: a randomized trial
Article information

Abstract
Background
The caudal route is a common approach for postoperative analgesia; however, it is associated with limited duration of action. The quadratus lumborum block (QLB) may produce prolonged postoperative analgesia. Therefore, this study aimed to compare the postoperative analgesic efficacy of the ultrasound-guided caudal block with that of the ultrasound-guided transincisional QLB (TiQLB) in pediatric patients undergoing open renal surgery.
Methods
Forty patients of both sexes, aged 2–11 years, were randomly assigned to receive either caudal analgesia with 1.25 ml/kg of bupivacaine 0.2% (Caudal group; n = 20) or a QLB with 0.5 ml/kg of bupivacaine 0.2% (TiQLB group; n = 20) in addition to standard general anesthesia. Time to first analgesia was the primary outcome. Total analgesic consumption in the first 24 h postoperatively, pain scores, and the incidence of side effects were the secondary outcomes.
Results
The mean time to first analgesic requirement was significantly longer in the TiQLB group than in the Caudal group (18.8 ± 5.1 vs. 6.7 ± 0.7 h, P < 0.001). Total ketorolac consumption and pain scores were significantly lower in the TiQLB group (P < 0.001). A few cases of mild postoperative nausea and vomiting were noted among patients in both groups; however, the difference was not statistically significant. No incidence of pruritus, shivering, or respiratory depression was noted.
Conclusions
Analgesia after the ultrasound-guided TiQLB with bupivacaine was superior to that after the ultrasound-guided caudal block, with similar side effects.
Introduction
Most pediatric renal procedures are reconstructive and require highly experienced laparoscopists. However, the indications for open pediatric renal surgery include nephrectomy [1], partial nephrectomy [2], pyeloplasty [3], and rare cases of renal stones [4,5]. The most common anesthetic technique in pediatric open renal surgery includes general anesthesia (GA) in combination with a regional analgesic block with patients in the lateral decubitus position to ensure that the airway is maintained. This combination reduces GA requirements, postoperative pain, and opioid use [6].
Administering a caudal epidural block using the landmark approach continues to be the most common regional anesthetic procedure performed under GA in pediatrics [7]. Caudal analgesia is recommended for pain relief during surgical procedures from the midthoracic to the lumbosacral dermatomes, including the urogenital tract, pelvis, and perineum [7]. Furthermore, the evolution of ultrasonography techniques has contributed to the accurate placement of blocks, particularly in infants with sacral anomalies [8]. Caudal blocks can promote early ambulation and hemodynamic stability during the postoperative period [9]. However, the duration of caudal analgesia may be insufficient to control postoperative pain [10].
A truncal block may result in prolonged postoperative analgesia. In 2007, the quadratus lumborum block (QLB) was first described by Chin et al. [11] as an effective method for postoperative analgesia in various surgeries, including renal surgeries. There are four main approaches to QLB: lateral, anterior, posterior, and intramuscular. A trans-incisional quadratus lumborum block (TiQLB), in which the local anesthetic is administered anterior to the muscle and results in the spread of the anesthetic solution between the quadratus lumborum muscle (QLM) and psoas major muscle (PMM), has also recently been described [12].
The results of a recent meta-analysis suggests that the QLB may be a useful postoperative analgesic strategy for children following lower abdominal surgery [13]. However, the TiQLB approach has not been investigated in the pediatric population. Hence, this study aimed to evaluate the effectiveness of ultrasound-guided caudal epidural blocks versus ultrasound-guided TiQLBs in reducing pain after elective open renal surgery in pediatric patients receiving GA.
Materials and Methods
This prospective, randomized study was performed at the urology unit of Ain-Shams University Hospital between March 2021 and October 2022 after it was approved by the Research Ethical Committee of the Faculty of Medicine at Ain-Shams University (code number: FMASU R 48/2020/2021), registered at the ClinicalTrials.gov database (registration number: NCT04790318), and informed consent was obtained from the guardians of all the included patients. The study was conducted in accordance with the principles of the Declaration of Helsinki (2013). Forty patients of both sexes, aged 2–11 years, with an American Society of Anesthesiologists physical status (ASA-PS) classification of I or II who were scheduled to undergo open renal surgery in the lateral decubitus position (nephrectomy, partial nephrectomy, pyeloplasty, and complex kidney stones) were included.
Patients were not eligible to participate in the study if their parents or guardians refused to participate or if they met any of the following criteria: an ASA-PS score > II, contraindication to regional analgesic procedures, major illness, spine or chest wall deformity, prior history of renal surgery, coagulation abnormalities, infection at the injection site, or an allergy or contraindication to the study medication.
Children were randomly assigned to either the caudal or TiQLB group using computer-generated lists and the closed-envelope method in a 1 : 1 ratio. The patients in the Caudal group (n = 20) received a combination of GA and ultrasound-guided caudal analgesia (immediately after wound closure) with 1.25 ml/kg bupivacaine 0.2% (three parts 0.25% bupivacaine to one part saline), whereas the patients in the TiQLB group (n = 20) received a combination of GA and ultrasound-guided TiQLB with 0.5 ml/kg bupivacaine 0.2%. The maximum allowable volume in both groups was 20 ml.
Ultrasound-guided caudal block technique
After wound closure, the patient’s knees were raised while still in the lateral position, with the upper knee flexed more than the lower knee. A linear high-frequency ultrasound transducer (TOSHIBA, model USAP-770A, Japan) was positioned horizontally in the midline over the sacral cornu under aseptic conditions to obtain a transverse view of the sacral hiatus or the “frog-eye” appearance. A 5-cm, 22-gauge needle was advanced at 45° through the sacral hiatus between the two cornu until it pierced the sacrococcygeal ligament and a “pop” was felt. Subsequently, the transducer was turned longitudinally to obtain a sagittal view of the sacrum and sacral hiatus (Fig. 1). The needle was then advanced in-plane through the sacral canal under real-time ultrasound guidance, and incremental doses of local anesthetic solution (1.25 ml/kg bupivacaine 0.2%) were injected after careful aspiration to rule out venipuncture or dural puncture.
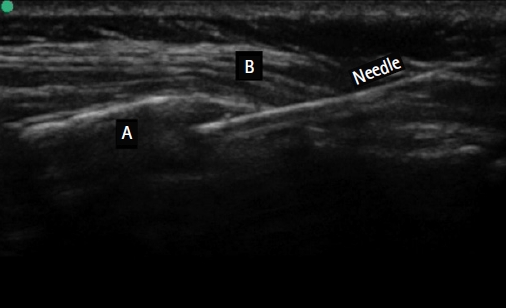
Ultrasound-guided caudal block, longitudinal axis. A: sacral canal, B: sacroccocygeal ligament.
Ultrasound-guided trans-incisional quadratus lumborum block technique
The TiQLB was performed after the surgery was completed but before the incision was closed. Retractors were used to open the surgical field while the patient was still in the lateral position with the surgical side up to provide a clear view of the QLM and PMM (Fig. 2A). All infection control precautions and instructions were strictly followed. The surgeon re-scrubbed the area, while the anesthesiologist wore a sterile gown and gloves, and used a sterile needle. A sterile, insulated convex ultrasound probe (5–8 MHz) (TOSHIBA, Model USAP-770A, Japan) covered with a TegadermTM film was placed 1 cm from the lateral edge of the incision above the QLM at the level of L2 until the shamrock sign was visualized (Fig. 2B). A 5-ml 22-gauge needle was inserted into the junction between the QLM and PMM in the anteromedial to posterolateral direction to penetrate the covering thoracolumbar fascia. Aspiration was carefully performed to ensure that the needle was not inside a blood vessel. A local anesthetic solution of 0.5 ml/kg bupivacaine 0.2% was slowly injected, and hydrodissection of the solution between the muscles was observed on ultrasound.
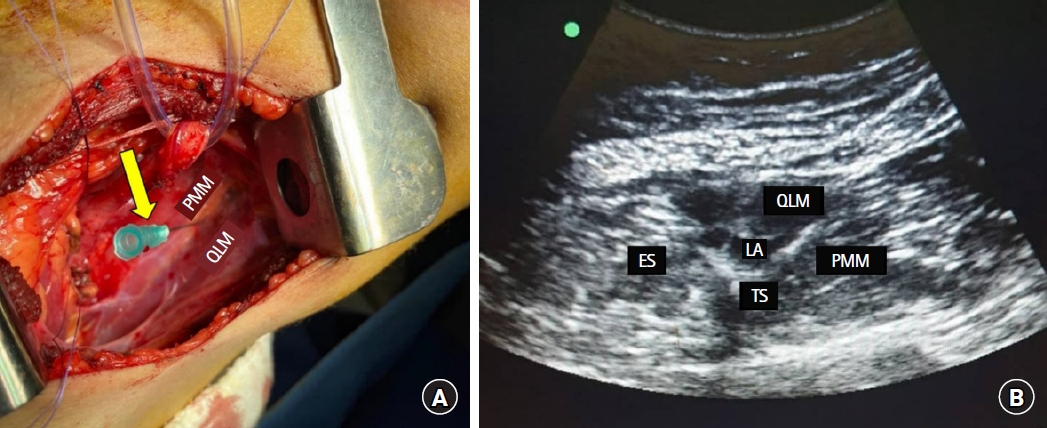
Trans-incisional quadratus lumborum block. (A) Arrow points to the needle between the QLM and PMM, piercing the anterior thoracolumbar fascia. (B) Ultrasound image of the quadratus lumborum block. ES: erector spinae muscle, LA: local anesthetic solution, QLM: quadratus lumborum muscle, PMM: psoas major muscle, TS: transverse lumbar spine.
The day before surgery, the patients underwent a comprehensive preoperative evaluation, including a full history, physical examination, and laboratory tests. Additionally, the parents or guardians were instructed to ensure that the patients fasted (6 h for solid food and 2 h for clear fluids) before anesthesia according to institutional policy. Thirty minutes before surgery, all patients were premedicated with oral midazolam 0.25 mg/kg (to a maximum of 15 mg) and the sedation level was closely monitored. Standard monitoring, including electrocardiography, noninvasive blood pressure measurements, and pulse oximetry, was initiated upon arrival in the operating room. Baseline readings were obtained for heart rate (HR), mean arterial pressure (MAP), and SpO2.
In both groups, preoxygenation was provided for 5 min before GA, and inhalation induction using 8% sevoflurane in 100% oxygen was administered via a sealed face mask. After the patient lost consciousness, a 22-gauge peripheral venous cannula was secured, propofol (1 mg/kg) was administered intravenously to deepen the level of anesthesia, and atracurium (0.5 mg/kg) was administered intravenously to assist with endotracheal intubation. Fentanyl was administered at a dose of 1 µg/kg. After securing the endotracheal tube, capnography was used to monitor end-tidal CO2, and the volume-controlled pressure-assisted mode of ventilation was adjusted to maintain normocapnia (CO2 35–40 mmHg). All patients received Ringer’s solution at a rate of 10 ml/kg/h. Additional fluid boluses (10–20 ml/kg) were administered as needed during the operation.
Atracurium supplementation (0.01 mg/kg), and isoflurane (1.5% minimum alveolar concentration) were used to maintain anesthesia. The patient was slowly and carefully placed in the lateral decubitus position with the surgical side facing up. During positioning, the vital signs (HR, MAP, and SpO2) were closely monitored to prevent serious adverse events. Hemodynamic monitoring (HR and MAP) continued intraoperatively, with readings obtained every 5 min, and any adverse events, such as bradycardia or hypotension, were promptly treated. For intraoperative analgesia, fentanyl was administered intravenously at incremental doses of 0.5 µg/kg and titrated according to the hemodynamic response to the surgical incision to maintain the HR and MAP within ± 20% of the pre-incision values with a maximum dose of 2 µg/kg. The bispectral index was used to measure the depth of anesthesia during the procedure and was maintained between 40 and 60 in both groups by controlling the isoflurane concentration.
At the end of surgery, patients were randomly assigned to receive either an ultrasound-guided caudal block or ultrasound-guided TiQLB. The blocks were performed by a consultant anesthesiologist with 20 years of experience administering pediatric regional nerve blockades.
In both groups, vital data were monitored closely during the injection of local anesthetics for any signs of toxicity, taking care not to exceed the maximum recommended dose (2 mg/kg bupivacaine). Intraoperative complications, such as damage to the underlying structures and hematoma formation were identified, and any signs of hemodynamic instability or local anesthetic toxicity were documented.
At the end of surgery, inhalational anesthesia was discontinued, gentle oral suction was performed, and reversal agents (atropine 0.02 mg/kg and neostigmine 0.04 mg/kg) were delivered once the patient recovered from the neuromuscular blockade and spontaneous breathing had resumed.
Subsequently, the patients were admitted to the post-anesthesia care unit (PACU), where they were followed up by an anesthesiologist and a nurse who were blinded to the study methodology. In the PACU, hemodynamic parameters were recorded immediately upon arrival and 20 and 30 min postoperatively. Once patients met the standard discharge criteria, they were transferred to the ward. A blinded observer anesthesiologist used the face, leg, activity, crying, and consolability (FLACC) scale [14] to assess the patients’ pain during the first 24 h (ranging from 0 to 10, where 0 = no pain and 10 = worst pain), at the time of arrival in the PACU, and regularly during the postoperative period. When the FLACC score reached ≥ 4, intravenous ketorolac was administered at a dosage of 0.5 mg/kg and repeated every six hours if the score remained ≥ 4 until oral intake was tolerated. The maximum daily dose of ketorolac was 90 mg, and the maximum treatment duration was 48 h. The time to first analgesic requirement and total ketorolac consumption over the first 24 h postoperatively were recorded.
The incidence of postoperative nausea and vomiting (PONV), which was categorized as none, mild, moderate, or severe, was documented for the first 24 h after surgery. Ondansetron 0.1 mg/kg was administered intravenously to treat PONV as needed. All other adverse events were also documented, including pruritus, shivering, and respiratory depression (respiratory rate < 10 breaths/min).
The primary outcome was the time to first analgesic requirement. The total amount of analgesics used in the first 24 h postoperatively, pain scores, and adverse events associated with the drugs or techniques used were the secondary outcomes.
Sample size calculation
The sample size was calculated using the STATA program (version 12, StataCorp LP, USA). The type-1 error (α) was set to 0.05 and the power (1-β) was set to 0.9. Results from a previous study [15] showed that 68% of the caudal block group required analgesia in the first 24 h compared to 7.5% in the QLB group. Using these values, we calculated 20 cases per group, taking into account dropouts and failed cases.
Statistical methods
The IBM Statistical Package for Social Sciences (SPSS) statistics software (version 22.0, IBM Corp., USA) was used to code, tabulate, and statistically analyze the obtained data. After checking for normality using the Shapiro-Wilk test, an independent t-test was conducted to compare normally distributed quantitative data, represented as the mean ± standard deviation (SD). The chi-square test was used to compare qualitative data, expressed as numbers and percentages, and Fisher’s exact test was used for variables with small expected numbers. Rates were compared using the log-rank test. Statistical significance was set at P < 0.05.
Results
Fifty-eight patients met the eligibility criteria for the study, 18 of whom were excluded because they did not meet the inclusion criteria (n = 14) or declined to participate (n = 4). Thus, 40 patients (20 per group) were included in the study and analyzed (Fig. 3). No statistically significant differences were noted between the groups in terms of demographic data (age, weight, sex, and ASA-PS classification), type of surgery, or operation duration (Table 1).
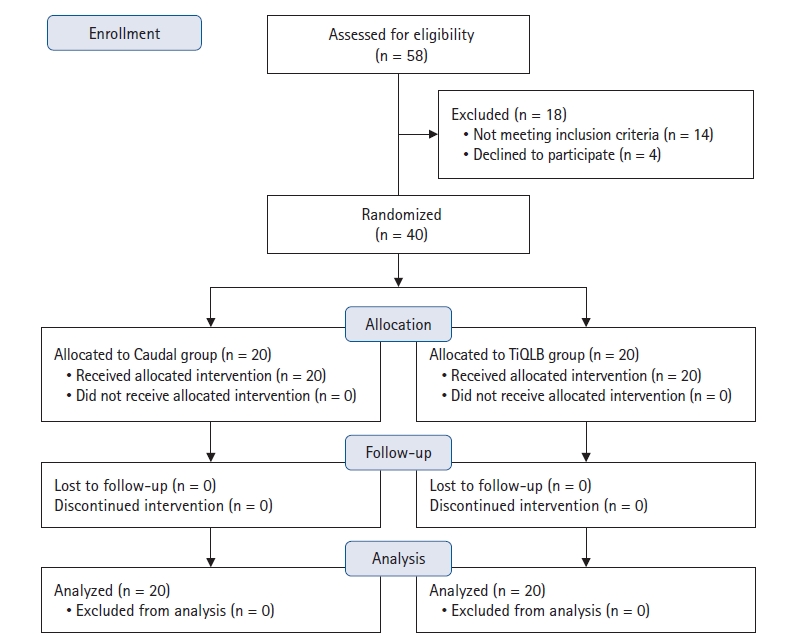
Consolidated Standards of Reporting Trials (CONSORT) flow diagram of patient selection. TiQLB: transincisional quadratus lumborum block.
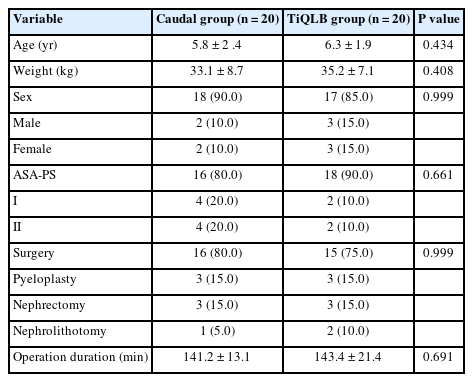
Comparison of Demographic Data, Type of Surgery, and Operation Duration between the Study Groups
No statistically significant differences in the mean hemodynamic parameter values (MAP and HR) intraoperatively (baseline, after intubation, mid-operatively, and 10 min post-block) or postoperatively (at 0, 20, and 30 min) between the groups were noted (Figs. 4A and B).

Comparison of hemodynamic parameters between the study groups. (A) Mean arterial pressure (mmHg). (B) Heart rate (beats/min). Lines are the mean data, and the error bars are the SD. TiQLB: transincisional quadratus lumborum block, HR: heart rate, MAP: mean arterial pressure, PO: postoperative.
The postoperative analgesia requirement rate (Fig. 5) and number of analgesic doses was significantly lower in the TiQLB group than in the Caudal group (P < 0.001). Eighty percent of the patients (n = 16) in the TiQLB group required no analgesic doses in the first 24 h postoperatively (20% of the patients [n = 4] in the TiQLB group asked for analgesia once). In contrast, all patients (n = 20) in the Caudal group requested analgesia during the same period (70 percent of patients [n = 14] in the Caudal group requested analgesia once and 30 percent of patients [n = 6] requested analgesia twice). The mean time to the first analgesic requirement among patients who required analgesia in the first 24 h postoperatively was longer in the TiQLB group than in the Caudal group (18.8 ± 5.1 h vs. 6.7 ± 0.7 h, respectively), with a statistically significant difference (estimated mean difference: 12.1 h, 95% CI [9.8, 14.3], P < 0.001) (Table 2).
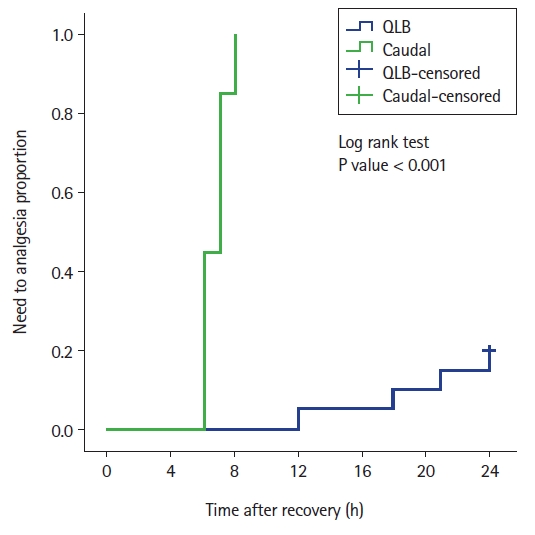
Kaplan-Meier curve for the postoperative analgesia requirement rate among the study groups; the log-rank test was used to compare the rates. QLB: quadratus lumborum block.

Comparison of Postoperative Analgesia during the First 24 h Postoperatively between the Study Groups
Additionally, the total ketorolac consumption was significantly lower in the TiQLB group than in the Caudal group (estimated difference: −18.3 mg, 95% CI [−24.7, −11.9], P < 0.001) (Table 2). Patients in the Caudal group had higher mean pain scores at 6, 10, and 12 h postoperatively (P < 0.001) (Fig. 6).
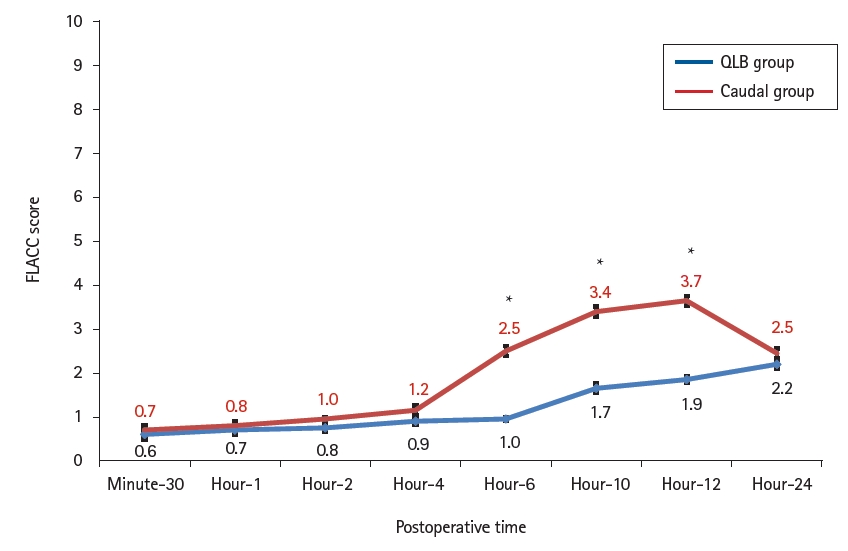
Comparison of the pain perception (FLACC-10) score between the study groups. Lines represent the mean data, and the error bars are the SD. *P < 0.001 compared to the control group. TiQLB: transincisional quadratus lumborum block, FLACC: face, leg, activity, crying, consolability.
Regarding postoperative adverse events, mild PONV was reported among patients in both groups, but the difference was not statistically significant (6 patients in the TiQLB group [30%] vs. 7 patients in the Caudal group [35%]; RR: 0.86, 95% CI [0.35, 2.10], P = 0.736). No incidence of pruritus, shivering, or respiratory depression was recorded. Furthermore, no hematoma or damage to the underlying structures associated with regional block administration and no incidents of local anesthetic toxicity or hemodynamic instability were recorded.
Discussion
The present study showed that the ultrasound-guided TiQLB is easy to administer, safe for the pediatric population, and provides a longer period of postoperative analgesia than ultrasound-guided caudal blocks, with a similar incidence of adverse events. To the best of our knowledge, this is the first study to examine the effects of ultrasound-guided TiQLBs in pediatric patients.
The caudal epidural block is the most commonly used regional technique in the pediatric population [16]. This block was originally developed as a blind landmark-based technique [17,18]. The ultrasound-guided caudal block, which was first described in 2003 by Klocke et al. [19], allows for the identification of small anatomical structures and visualization of the spread of the local anesthetic [20–22]. According to a recent Cochrane Review [23], this technique increases the block duration in young children and improves success rates.
Despite these advantages, the relatively short duration of analgesia remains a concern for caudal blockade. To improve the duration of action of local anesthetics, adjuvants such as narcotics, ketamine, and α2-receptors have been used with good results. However, concerns regarding associated side effects have been expressed [9].
The introduction of truncal blocks such as the transversus abdominis plane (TAP) and QLB has shown more favorable results in the pediatric population. According to Baidya et al. [24], a single injection of transmuscular QLB in pediatric patients undergoing pyeloplasty is associated with satisfactory postoperative analgesia. Moreover, according to Murouchi [25], analgesia is significantly prolonged after laparoscopic appendectomy in pediatric patients undergoing bilateral intramuscular QLB. Oksuz et al. [26] also found that QLB could be a superior alternative to TAP blocks in terms of postoperative analgesia, pain scores, and parental satisfaction (P < 0.05).
In this study, the TiQLB produced postoperative analgesia that lasted significantly longer than that produced by the ultrasound-guided caudal block. In addition, ketorolac requirements were significantly lower among the patients in the TiQLB group. The anterior QLB, which is similar to our TiQLB, may extend cephalad to reach the T7–T12 spinal nerve roots, which could explain the efficacy of the QLB [27]. In contrast, the nature of the epidural space may contribute to the short duration of caudal analgesia in pediatric patients because it is characterized by high vascularity, which leads to rapid absorption of local anesthetics [28]. A recent meta-analysis reported a duration of caudal anesthesia that was shorter compared to other peripheral nerve blocks in hypospadias surgeries, as well as higher pain scores and analgesic consumption [29].
In accordance with the present results, Oksuz et al. [15] assessed the analgesic effect of the ultrasound-guided QLB compared with the ultrasound-guided caudal block in inguinal hernia repair and orchiopexy procedures in pediatric patients and demonstrated a lower analgesic requirement in the first 24 h in the QLB group (P = 0.001). Additionally, postoperative FLACC scores at 4, 6, and 12 h were significantly lower in the QLB group (P = 0.001). In another study, Sato [30] observed similar results in pediatric patients undergoing vesicoureteric reflex surgery, in which the QLB was more effective than caudal ropivacaine/morphine in reducing the need for opioid-based rescue analgesia during the first 24 h.
However, İpek et al. [31] reported contrasting results in their study investigating perioperative analgesic options for pediatric patients undergoing lower abdominal surgery, including the ultrasound-guided TAP block, QLB, and caudal analgesia. In their study, QLB was associated with lower postoperative pain scores and shorter hospital stays; however, no statistically significant difference was found between the groups in terms of the time to the first analgesic requirement or the number of patients requiring analgesia within the first 24 h after surgery [31]. This discrepancy may be attributed to the use of a different QLB approach (posterior QLB).
Regarding the incidence of adverse events in the present study, no cases of pruritus, shivering, respiratory depression, or complications related to block administration was reported. Only a few cases of mild PONV were reported among patients in both groups, with no statistically significant difference. In addition, the administration of regional blocks did not result in hematoma, injury to underlying structures, local anesthetic toxicity, or hemodynamic instability. The low incidence of adverse events may be attributed to the relatively small sample size and the fact that the TiQLB allows for direct visualization of the needle during insertion.
Analysis of the Pediatric Regional Anesthesia Network database reported complications associated with 18,950 caudal blocks, including block failure (1%), blood aspiration (0.6%), dural puncture (0.08%), cardiac arrest (0.005%), seizures (0.005%), and sacral pain (0.005%). As most of these complications were likely related to local anesthetic toxicity, the authors recommended that adjustments in the drug dosage could render the procedure safer [32].
Few reports on QLB-related complications such as local anesthetic toxicity, organ injury, and retroperitoneal hematoma are available in the literature. However, hemodynamics must be closely monitored because local anesthesia can spread to the paravertebral area, causing the HR and blood pressure to decrease [33]. One case report described femoral block-induced weakening of the quadriceps, which disappeared after 18 h [34]. In the current study, no significant changes in hemodynamics were noted, and none of the patients in the TiQLB group exhibited quadriceps muscle weakness.
The current study had some limitations. First, because the ultrasound-guided TiQLB requires an incision, it cannot be prescribed to all patients. Second, because the current study was based on administering blocks to pediatric patients undergoing GA, we were unable to examine the dermatomal levels after the procedure in either group.
In conclusion, this study aimed to identify a more effective postoperative analgesic method for open renal surgery in pediatric patients. Analgesia after the ultrasound-guided TiQLB with bupivacaine was superior and more effective than that after the ultrasound-guided caudal epidural block, with similar side effects and hemodynamics.
Notes
Funding
None.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
Amin M. Alansary (Conceptualization; Data curation; Investigation; Methodology; Supervision; Validation; Writing – original draft; Writing – review & editing)
Atef Badawy (Data curation; Investigation; Methodology; Resources; Validation; Writing – review & editing)
Marwa A. K. Elbeialy (Data curation; Investigation; Methodology; Supervision; Validation; Writing – original draft; Writing – review & editing)