Arytenoid dislocation after uneventful endotracheal intubation: a case report
Article information
Abstract
Arytenoid dislocation is an unusual complication of endotracheal intubation. We reported a case of a 48-year-old female with arytenoid dislocation after uneventful endotracheal intubation, which was successfully treated with arytenoid reduction. The patient complained of persistent hoarseness until the fourth day after an uneventful gynecologic surgery under general anesthesia. On laryngoscopic examination, paralyzed left vocal cord with minimal arytenoid movement was observed. An anteromedial dislocation of the left arytenoid cartilage was suspected and surgical reduction was performed by the laryngologist. The hoarseness was immediately resolved after surgical intervention. Anesthesiologists should be careful not to cause laryngeal trauma in anesthetized patients. In addition, early diagnosis and prompt surgical reduction are essential for a better prognosis for arytenoid dislocation.
All procedures performed to secure the airway can cause laryngeal morbidity, such as hoarseness, submucosal hemorrhage, subglottic edema, laryngitis, and arytenoid cartilage dislocation [12]. Among others, hoarseness is reported as the most common laryngeal morbidity after general anesthesia, with widely varying incidence from 16% to 55% [3]. However, it is generally resolved within a few days, unless accompanied by serious complications, such as arytenoid dislocation [3].
The arytenoid cartilages are a pair of small 3-sided pyramids that form part of the larynx, to which the vocal cords are attached. Arytenoid dislocation is an unusual complication after external trauma or endotracheal intubation; its incidence is < 0.1% when associated with intubation [4]. Iatrogenic arytenoid dislocation is occasionally reported in cases with difficult intubation, double lumen endotracheal tube intubation, or intubation with a stylet [56]. However, we experienced a case of arytenoid dislocation despite easy and uneventful intubation. Therefore, we reported this case along with a review of related literature.
Case Report
A 48-year-old female of 163 cm height and 55 kg weight was scheduled for an open radical hysterectomy and bilateral pelvic lymph node dissection. Her physical and laboratory examinations were unremarkable, with an American Society of Anesthesiologists I preoperative physical status classification. Her Mallampati score was I, and her mouth opening and thyromental distance were normal. She did not report a history of chronic renal failure, diabetes mellitus, corticosteroid use, laryngomalacia, or acromegaly.
Anesthesia was induced by the resident anesthesiologists on duty under the supervision of an experienced anesthesiologist with a continuous target-controlled infusion of 5 µg/ml of propofol and 3 ng/ml of remifentanil. After loss of consciousness that was confirmed by Bispectral Index score (BIS, Covidien, Mansfield, MA, USA), 7 mg of vecuronium was injected for intubation. After 4 min, without using stylet, an ID 7.0 mm plain endotracheal tube was smoothly inserted into the patient's trachea without difficulty under direct laryngoscopic view (Macintosh 3 laryngoscope blade) upon first attempt. The epiglottis was short, but the glottis was Cormack-Lehane Grade I. The patient did not cough or move during the intubation. The tube was fixed at the right lip corner and secured properly with the tube holder. After anesthetic induction, the patient was carefully moved caudally for surgical positioning. Otherwise, she was not moved, because the operation was open laparotomy, which is performed in only supine position without any required movement of the operating bed. Besides, there was no movement of head and neck to place intravenous catheters. An esophageal stethoscope (18 Fr, DeRoyal Industries, Powell, TN, USA) was inserted for temperature monitoring and a nasogastric (NG) tube (18Fr, INSUNG Medical, Co., Daegu, Korea) was inserted at the surgeon's request. A resident anesthesiologist inserted the NG tube and esophageal stethoscope without reporting any difficulty.
During the 4 hour operation, anesthesia was maintained with propofol, remifentanil, and vecuronium. The surgery was uneventful, and after the operation, the endotracheal tube cuff was deflated and the patient was extubated; severe coughing did not occur during the emergence. During the stay in post anesthesia care unit (PACU), she did not complain of any symptoms such as hoarseness or laryngeal pain. On the first postoperative day in the ward, she complained of moderate hoarseness. The physician expected the symptom would resolve spontaneously, but the patient complained of persistent hoarseness on the fourth day after the operation. There were no symptoms other than hoarseness. On the sixth day after the operation, fiber-optic laryngoscopy was performed by the laryngologist.
On laryngoscopy, the left vocal cord was fixed in the paramedian position, however minimal movement of arytenoid during phonation was observed. The left vocal cord did not show any movement even following a deep inspiration. Left arytenoid was placed with anteromedial side. A difference in level between the 2 vocal cords caused by the infra-placement of the left vocal cord was observed (Fig. 1). Arytenoid dislocation was suspected, and surgical reduction under general anesthesia was scheduled.
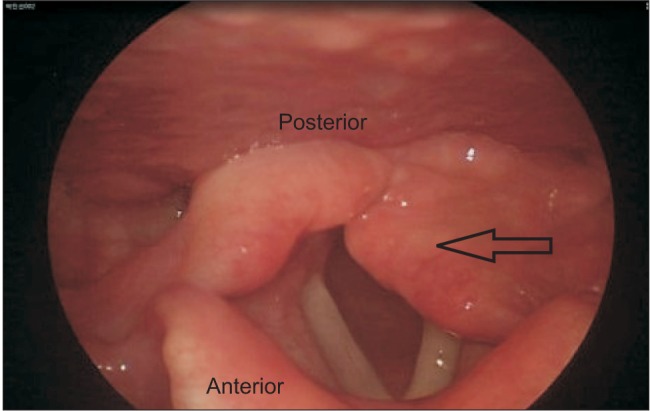
Laryngoscopic finding of anteromedial dislocation of left arytenoid cartilage.
Reduction was attempted by repeatedly applying force to the left arytenoid cartilage toward the posterolateral side using the peanut surgical instrument (Sipjasung Wize, Co., Seoul, Korea). After reduction and just before the patient woke from the anesthesia, the movement of the both vocal cords was confirmed under direct laryngoscopic view (Macintosh 3 laryngoscope blade). The patient's voice was improved immediately after the surgery; and a month after the surgery, movement of the vocal cords was completely normal. Fig. 2 showed an image taken 3 weeks after surgical reduction. Written informed consent was obtained from the patient for publication of this case report and the accompanying images.
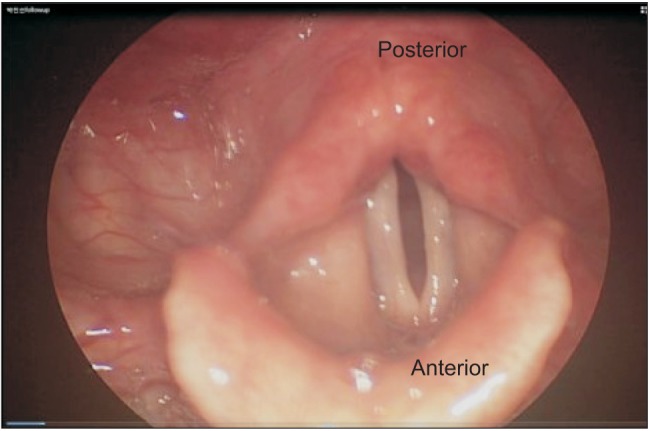
Laryngoscopic finding of vocal cord at 3 weeks post-surgical reduction.
Discussion
Postoperative arytenoid dislocation is an unusual complication after general anesthesia and is thought to be related to a difficult or traumatic intubation [167]. The predisposing factors are laryngomalacia, renal insufficiency, acromegaly, or chronic glucocorticoid intake, which might weaken the cricoarytenoid joint [8]. In our case, the patient had no predisposing factors and was intubated cleanly and smoothly without any event. Similarly, there are earlier reports of arytenoid dislocation after uneventful endotracheal intubations [89].
NG tube or esophageal stethoscope insertion should be conducted carefully and gently in anesthetized patients to avoid laryngeal trauma. These procedures can cause arytenoid dislocation, because arytenoid cartilage is one of the most common sites of resistance when inserting NG tube [10]. Esophageal stethoscope can also cause arytenoid dislocation for the same reason; however, there are no specific case reports of esophageal stethoscope or a NG tube insertion-induced arytenoid dislocation. In our case, NG tube and esophageal stethoscope were inserted by a highly skilled anesthesiologist with no reported difficulty. However, it is possible that he did not recognize that some resistance felt during the insertion could have been a "difficulty" at all or a cause of laryngeal trauma. Placing NG tube and esophageal stethoscope back and forth inside the patient's larynx can often occur without regarding that the subtle resistance felt during insertion can present a tremendous hazard to the patients. Therefore, there is a possibility of hidden laryngeal trauma from these apparently uneventful procedures. Other possible causes can be assumed as follows.
Performing intubation in incompletely relaxed state can be a causative factor of laryngeal morbidities. The quality of tracheal intubation reportedly decreases and laryngeal morbidity increases without complete muscle relaxation [11]. Mencke et al. reported that when performing intubation, the group with suboptimal muscle relaxation has more post-operative laryngeal morbidities such as hoarseness, laryngeal hematoma, granuloma, or thickened mucosa. In our case, tracheal intubation was performed 4 min after the injection of an adequate dose of vecuronium. However, despite the assumed complete muscle relaxation, optimal muscle relaxation for tracheal intubation was not assessed objectively in our case. To confirm complete muscle relaxation and determine the best timing for tracheal intubation, neuromuscular monitoring, such as train-of-four watch is necessary, which can decrease the incidence of laryngeal damage [11].
During the operation, movement or the inappropriately secured position of the endotracheal tube could be factors causing arytenoid dislocation [11]. In our case, the patient was moved caudally once for surgical positioning. The anesthesiologist is required to grip the endotracheal tube when moving the patient to avoid trauma to the vocal cord structures, as was followed in our case.
Furthermore, severe coughing or extubation with a non-deflated cuff during emergence could be potential causes of arytenoid dislocation. Severe coughing during the emergence period can cause laryngeal morbidity, such as arytenoid dislocation, but it was not clear in our patient. Although the exact pathomechanism of arytenoid dislocation is unknown, posterior dislocations of arytenoid cartilage can be caused by trauma during extubation, while anterior dislocations occur during intubation [1]. Therefore, performing extubation with a non-deflated cuff is a potential risk factor for traumatic extubation and arytenoid dislocation, as well [1]. Our patient had an exact anteromedial arytenoid dislocation, and not posterior dislocation. Therefore, it is possible that intubation is a more reasonable factor in the etiology than traumatic extubation.
The primary symptom of arytenoid dislocation in adults is persistent hoarseness [13]. Some symptoms, such as dysphagia, sore throat, and stridor, may be present [7]. In our case, the patient complained only of prolonged hoarseness for 6 days after the operation. However, the definition of "prolonged" with respect to hoarseness can be controversial. One study reported that hoarseness occurs in almost half of the patients on the day of operation, but hoarseness lasting 1 week is unusual [3].
Neck computer tomography (CT) and electromyography (EMG) can often be helpful for diagnosing arytenoid dislocation [12]. Like arytenoid dislocation, nerve damage from a variety of etiologies such as intra-operative laryngeal mucosal ischemia, can cause temporary vocal cord paralysis and resulting hoarseness. It is important to differentiate arytenoid dislocation from nerve damage, because while nerve damage from mucosal ischemia needs conservative treatment, arytenoid dislocation needs immediate surgical reduction. However, in our case, the patient had paralysis of the glottis, which occurred after a gynecologic surgery and was unrelated to intraoperative damage of the vagus nerve. The paralysis of the glottis can be caused by either nerve damage resulting from the pressure of the endotracheal tube due to prolonged surgery time or arytenoid cartilage dislocation. Because it is not easy to distinguish between the 2 with clinical findings alone, Larynx CT and EMG is required [12]; however, these are no tools for definite diagnosis [1]. Suspicion based on clinical findings and circumstances is most important to the diagnosis of arytenoid cartilage dislocation [112]. Arytenoid cartilage dislocation was suspected more than vagus nerve damage in the current patient, because of the minimal movement of the arytenoid cartilage and level difference of both vocal cords.
Once diagnosed, immediate surgical reduction under general anesthesia is the treatment of choice [12]; in addition, early diagnosis increases the likelihood of successful surgical reduction and a good functional outcome [13]. Furthermore, surgical reduction is still the best option for arytenoid cartilage dislocation even when the diagnosis is delayed. Injection laryngoplasty or botulinum toxin is applied if surgical reduction is not successful [14], and sometimes even more invasive surgical procedures, such as open arytenoid reduction operation or Type I thyroplasty are indicated if the diagnosis and optimal treatment are delayed [1]. In our case, arytenoid dislocation was diagnosed relatively early and surgical reduction was performed successfully.
In conclusion, we reported a case of arytenoid dislocation after an uneventful intubation but assumed traumatic nasogastric tube and esophageal stethoscope insertion. Anesthesiologists should be careful not to cause laryngeal trauma in anesthetized patients when performing procedures around the airway. In addition, because early diagnosis and prompt surgical reduction are crucial for a better prognosis for arytenoid dislocation, if hoarseness persists for more than a week after operation, the clinician should suspect a serious complication like arytenoid dislocation. Further evaluations and treatment should be performed immediately.