Cannulation of the dorsal radial artery: an underused, yet useful, technique
Article information
Arterial cannulation is an essential technique, especially during surgery with substantial hemodynamic changes or involving complex procedures. Among various vascular sites, the radial artery is the preferred route of access. However, when this is unsuccessful, the most appropriate alternative site has not been established. We report a case of dorsal radial artery cannulation after failed radial artery cannulation, in a patient undergoing kidney transplantation.
A 29-year-old male patient was referred for living donor kidney transplantation surgery. He was diagnosed with IgA nephropathy previously, which was initially managed with medications. For the past 1½ years, he has been receiving hemodialysis because of poor compliance with medications. No other past medical history, including peripheral vascular disease, was noted.
Anesthesia was induced after placement of electrocardiogram leads, a pulse oximeter, a noninvasive blood pressure monitor, and a bispectral index monitor. Propofol (2 mg/kg) and atracurium (0.5 mg/kg) were injected intravenously, and endotracheal intubation was performed. Anesthesia was maintained with desflurane 5.0-6.0% in 50% oxygen with air and a continuous infusion of remifentanil. An Allen's test was performed to confirm the presence of a patent collateral blood supply to that hand. Arterial cannulation for continuous arterial blood pressure monitoring was attempted twice in the patient's right radial artery, but was unsuccessful. Because of vasospasm and a substantial hematoma in the volar aspect of the wrist caused by the unsuccessful cannulation attempts, alternative sites for arterial cannulation were sought. The dorsal radial artery was located by palpation of the pulse on the dorsum of the hand, between the bases of the first and second metacarpals, in the "anatomical snuffbox." A 20-gauge angiocatheter (Biosafety™ IV Catheter, Sewoon Medical Co. Ltd, Cheon-An, Korea) was inserted through the skin at a 30° angle, directly over the point at which the pulse was palpated, and when brisk blood return was obtained, the catheter was advanced slowly toward the pulse. After successful cannulation, the catheter was connected to a transducer and secured (Fig. 1A). During the surgery, blood sampling from the arterial line was performed four times and done without any difficulties or complications. The duration of surgery and anesthesia was 168 and 215 minutes, respectively, and the duration of arterial catheter maintenance was 234 minutes. The dorsal radial artery catheter was removed in the post-anesthesia care unit prior to transfer to the general ward; the site was manually compressed upon removal of the catheter to help achieve hemostasis. No complications related to the arterial cannulation, such as digital ischemia, pain, or paresthesias, occurred upon catheter removal or within the 13 days of hospital stay after surgery.
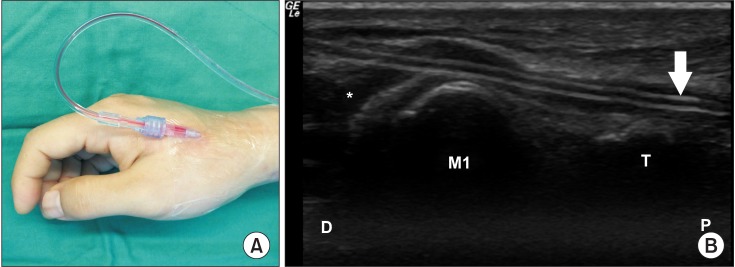
(A) Successful arterial cannulation in the dorsal radial artery. (B) Longitudinal ultrasound image showing arterial catheter (white arrow) placed within the dorsal radial artery (white asterisk). M1: first metacarpal bone, T: trapezium bone, D: distal, P: proximal.
Arterial cannulation is widely adopted monitoring technique, which provides vital information in the perioperative period and enables clinicians to respond appropriately to immediate changes in a patient's status. Among various vascular options for arterial cannulation, the radial artery in the volar aspect of wrist is generally preferred. The radial artery occupies a consistent and relatively straightforward position, and its superficial location enables easy palpation of the pulsation. In contrast with the well-established benefits of this popular site, the alternative after failure of the transradial approach remains controversial [1]. Alternative options include brachial, ulnar, or femoral arterial catheterization and the authors' alternative choice would be the brachial artery for its easy accessibility. But these methods have possible drawbacks, such as difficult access and maintenance because of the artery's tortuous course, catheter kinking, or atheroma formation, respectively [2]. Although cannulation of the dorsal radial artery has been introduced as one of the best alternatives when the transradial approach fails, it has not been widely used, and many clinicians have little knowledge about this method [3,4].
The digital arteries supplying the fingers arise from the superficial palmar arch. The palmar branch of the radial artery, which contributes to the superficial palmar arch, arises from the radial artery in the volar side of the wrist before entering the anatomical snuffbox. Catheterizing the dorsal radial artery has the advantage of cannulating more distally than with the traditional transradial approach, beyond the origin of the palmar branch. Avoiding trauma to this important collateral vessel could reduce the risk of digital ischemia. Moreover, maintaining vessel integrity both during and after cannulation could be advantageous when cannulating a branch located most distally from the aorta.
Although the radial artery in the volar area is favored for its superficial location, the dorsal radial artery is also superficially palpable within the anatomical snuffbox. The ease of accessibility and anatomical merits of the dorsal radial artery have been demonstrated by previous studies [3,4]. Moreover, whereas the course of the superficial radial artery on the volar side can be altered by even minor changes in wrist positioning, the dorsal radial artery is free from such positional influences. As the dorsal radial artery resides in the anatomical snuffbox, it is firmly positioned between the first dorsal interosseous muscle and extensor carpi radialis longus muscle, so a catheter within this artery will be in a stable position, with minimal risk of kinking or malpositioning, even after abrupt positional changes (Fig. 1B). This could be particularly advantageous when arterial catheterization is required in a hand already containing a venous catheter, especially if the catheter is on the dorsum of the hand. This situation is often encountered in patients with multiple limb fractures or those with a previous mastectomy with axillary lymph node dissection or chronic renal failure with an arteriovenous fistula in the opposite hand.
The radial artery is one of the most important arteries, not only in the fields of anesthesia, but also in various areas of medicine. It can function as an access route for percutaneous coronary intervention, a feeding artery for reconstructive flaps, a conduit for coronary artery bypass, the element in an arteriovenous fistula, and also as the monitoring artery for invasive blood pressure measurements. In conclusion, dorsal radial artery cannulation is a less known, but worth mastering, alternative choice for cannulation, which can easily be adopted when commonly used options are no longer available and a peripheral arterial site is preferred.