Introduction
The values espoused by an institution and the social support it provides are key determinants of employees’ level of engagement [1]. Workplace gender-based mistreatment (GBM) refers to any negative or harmful behavior directed towards an employee in a workplace setting [2]. GBM can take many different forms, including discrimination, abuse, and harassment. The presence of GBM in a healthcare setting can create a hostile work environment that may lead to job dissatisfaction and underperformance, potentially compromising patient outcomes and leading to burnout, depression, and other poor psychological outcomes, such as suicidality [3–7].
Rates of GBM vary among physicians, with studies reporting rates of harassment ranging from 18% to 50% [3,8], depending on the source within the healthcare setting. Current literature indicates that GBM is particularly common among surgical specialties, specifically among female surgeons and surgical residents [3,8–10]. Given that anesthesia is recognized as a high-stress medical specialty mainly due to a lack of control over the working schedule; poor interpersonal professional relationships; and poor recognition by surgical colleagues, the general public, and the media [11], it would be reasonable to assume that these issues also exist in the anesthesia community.
Indeed, prior research has established that GBM occurs in the workplace for anesthesiologists [12–14]. Sources of GBM among anesthesiologists include colleagues, surgeons, patients, visitors, and supervising physicians [3,14]. A recent survey demonstrated that female anesthesiologists perceived the attitudes of coworkers (including surgeons, patients, nurses, and other anesthesiology colleagues) towards them to be worse than those perceived by male anesthesiologists [14]. The odds being mistreated in the workplace was 10.6 times greater for female anesthesiologists than for male anesthesiologists, and women chose to report GBM in only 24% of cases. This may be due to the limited number of countries with gender policy statements in the field of anesthesia and unclear country-specific legal dispositions for workplace GBM offenders [15].
The aspects of the work environment that are associated with perceptions of workplace GBM among anesthesiologists in Europe and the differences among European countries are currently not clear. The aim of this study is to address this knowledge gap and explore the variables associated with workplace GBM among anesthesiologists in Europe and the specific countries that are more at risk of being subjected to these forms of work-related environmental stress. We expect this ranking to provide a basis for comparing different European countries and, more importantly, serve as a benchmarking tool for monitoring progress over time. In this study, the term “gender” refers to an individual’s gender identity, which is distinct from the sex assigned at birth. Gender identity refers to a person’s deeply felt sense of gender, regardless of whether it aligns with the sex they were assigned at birth. It encompasses one’s internal sense of being male, female, neither, or any other gender identity. It is important to differentiate between gender and sex assigned at birth, as the latter is based on biological attributes such as genitalia, while gender identity is a deeply personal and subjective experience.
Materials and Methods
Ethics
We conducted a secondary analysis of an existing database that assessed anesthesiologists' careers, including leadership and research opportunities, clinical work attitudes, and considerations for gender equality. The project underwent a rigorous ethical review process, provided by the Ethics Committee at the University Medical Center Maribor, Maribor, Slovenia (Chairperson, Associate Professor Milan Reljic, M.D., Ph.D.) and collected under Ref. UKC-MB-KME-75/19 on September 11, 2019. The data were maintained in accordance with the highest ethical standards, including measures to protect the participants’ confidentiality and privacy. A separate ethical approval was not required for the publication of the secondary analysis, as the Institutional Review Board review of the initial survey was considered adequate. Moreover, as part of the survey, the respondents explicitly granted permission for an analysis to be published. At the end of the survey, participants were presented with a comprehensive set of questions and informed about the research objectives. They provided informed consent for the use of their responses in the subsequent analyses. As this type of consent ensures that participants have a full understanding of how their data will be used, it is particularly robust and enhances the ethical foundation of our secondary analysis. This study complies with the CROSS EQUATOR reporting guidelines.
Participants
We conducted an international, internet-based, cross-sectional survey of anesthesiology physicians. Briefly, we used a 46-item questionnaire to assess anesthesiologists’ perceptions of leadership, research opportunities, and clinical work attitudes (Questionnaire – Supplementary Marterial 1). After a pilot was conducted and validated, the questionnaire was hosted online on SurveyMonkey®. It was then distributed through social media using the ‘snowballing’ sampling technique [16,17]. The survey was available from September 14, 2019 to October 26, 2019, and included 15,714 respondents from 148 countries. The survey completion rate was 80.8% [14]. We aimed to reduce selection bias by collecting at least 10% of the members of the national anesthesiology society for each country or at least five responses per million people [17]. An in-depth description of the survey development and distribution methodology has been published elsewhere [14].
In this secondary analysis, we examined the factors associated with workplace GBM among European anesthesiologists. The survey questionnaire consisted of several items assessing various aspects of gender bias and workplace mistreatment. We focused on the associations and potential predictors of GBM based on the survey responses to question 22: ‘Have you ever been mistreated at your workplace because of your gender?’ (Questionnaire – Supplementary Marterial 1). Importantly, the questions used as explanatory variables in our regression analyses are independent of the dependent variable (i.e., the presence of GBM). These questions primarily focus on demographic information and perceptions of gender-related disadvantages in leadership and research. As these questions were independent from the outcome variable, we were able to independently analyze their individual contributions to GBM. To ensure the validity of our regression models, we assessed the assumption of independence among the independent variables. This assessment was carried out both before and during the modeling phase. Before initiating regression modeling, we evaluated the potential correlations among the independent variables by computing the correlation matrices and creating scatterplots to visualize any relationships or associations among the independent variables. This pre-modeling assessment allowed us to identify any significant correlations that could affect the independence assumption. Throughout the modeling process, we employed variance inflation factor (VIF) analyses as an additional measure to quantify the degree of multicollinearity among the independent variables. High VIF values indicate problematic levels of multicollinearity that can affect the independence assumption of the regression models. We closely monitored the VIF values to ensure that our models met the independence criterion. Regardless, this assumption of independence would not have affected the validity of the regression analyses. We also recognize that additional factors or interactions not captured by these questions may also contribute to GBM, and further research should explore these factors in more detail.
We selected all respondents from European countries, as defined by the European Society of Anesthesiology and Intensive Care and the World Health Organization [18]. Demographic characteristics were assessed, including self-reported gender (woman, man, non-binary), age, and level of training.
Statistical analysis
A descriptive statistical analysis was conducted to determine the characteristics of the respondents. Proportions are reported for categorical variables. Parametric data are reported as mean ± SD and were analyzed using the Student’s t-test. Associations between GBM and the remaining variables were analyzed using univariate and multivariable logistic regression, with the goal of identifying independent predictors. Model fit was examined using the Cox & Snell R2 and Nagelkerke R2 of the variance in checklist completion. Statistical significance was set at P < 0.05. Receiver operating characteristic curves of the multivariate observations were plotted to assess the predictive performance of the logistic regression model. All the statistical analyses were performed using SPSS version 27 (IBM Corp.).
Generalized linear mixed models (GLMMs) were then developed to quantify the impact of GBM in each European country. We used GLMMs because they estimate fixed and random effects and are useful when the dependent variable is binary, ordinal, count, or quantitative but not normally distributed [19]. We developed several models using the fixed variables that were statistically significant in the prior logistic regression. Among all possible models, we chose the one with the lowest Akaike information criterion (AIC) because this would represent a better model fit. The AIC is an estimator of the prediction error and thereby the relative quality of a statistical model for a given dataset and is used to determine how well a dataset fits the data from which it was generated [20]. We assumed a binomial distribution for the GLMM estimation as this was the most appropriate for modeling the variability in our data, considering the nature of our response variable and the design of the study. We used the logit link function in the GLMM as the response variable was categorical.
Among the models with lower AICs, we chose the one with the fewest variables. The fixed-effect factor covariates in our chosen model were gender, ratio of women to men in the workplace, gender of the department head, and perception of gender as a disadvantage for leadership. The random variable was the country of practice. Fixed-effect factor covariates were estimated using an extended likelihood or first-order Laplace approximation of marginal probability [21]. This approach is suitable for non-Gaussian response distributions, and effectively handles random effects, ensuring accurate parameter estimations and precise GBM score predictions for European countries.
Using the “1 variable per 10 events” criterion, we excluded countries with fewer than 50 total responses. A total of 26 countries were thus included in the GLMM analyses. A random intercept for each country accounted for the intra-country correlations. The statistical significance of the analysis point covariate was tested using the drop in the deviation compared with the null model. The GBM value was analyzed in a manner consistent with its bounded range, acknowledging that the range of possible values associated with this variable was limited. For zero values, a marginal value of 0.001 was added to comply with the beta distribution range. All the analyses were based on the input dataset. For the GLMM, statistical significance was set at P < 0.05. Statistical analyses were performed using R and R Studio (R version 4.2.1., The R Foundation for Statistical Computing). The following R packages were used in our analysis: ggplot2 (version 3.3.3) [22], lme4 (version 1.1-27) [23], dplyr (version 1.0.6) [24], caret (version 6.0-88) [25], and foreign (version 0.8-82) [26].
Treatment of missing data and response consistency
Our approach to missing data involved the use of multiple imputation techniques to estimate the missing values. This method involves creating several datasets with imputed values for missing data points. The imputed datasets were generated based on the observed information and relationships within the dataset. We then analyzed these datasets and combined the results to consider the variability introduced by the imputation process. To maintain response consistency and ensure data quality, we implemented data validation checks and quality control procedures throughout survey administration and the data collection process. These measures included data validation checks, peer debriefing, and interim analyses. Automated data validation checks were integrated into the online survey platform to ensure that the respondents provided complete and internally consistent responses. For example, we used logic checks to confirm that responses to certain questions were consistent with previous answers or fell within a valid range. Our research team regularly engaged in peer debriefing sessions to collectively review and discuss the survey responses. This iterative process allowed us to identify and rectify any inconsistencies or discrepancies in the data. Finally, we conducted interim analyses in clusters of 1,500 responses for open-ended questions. This approach assessed data saturation and identified common themes and emerging patterns. These interim analyses helped us to refine our understanding of the data and maintain response consistency. We used complete case analysis, commonly referred to as listwise deletion, as our method for handling missing data during data analysis. To implement this approach, we first identified missing data for each variable of interest in our dataset. Cases or observations with any missing values for these variables were systematically excluded from the analysis, resulting in a dataset comprising only complete cases.
Results
In our analysis, we included responses from 43 European countries (n = 5,795) to investigate the factors associated with GBM in the workplace (Table 1). Univariate and multivariable logistic regression analyses were conducted to understand the impact of various factors on the likelihood of experiencing GBM.
The multivariable logistic regression model included four independent variables: age, gender, perception of gender as a disadvantage for leadership, and perception of gender as a disadvantage for research. We also considered interactions such as the ratio of women to men, number of female anesthesiologists per department, and their respective interactions (Supplementary Marterial 2). The full model, which contained all these predictors, was statistically significant (P < 0.001), demonstrating that it could distinguish between individuals who had and those who had not experienced GBM (for detailed logistic regression results, see Supplementary Marterial 2). Notably, female gender, younger age, and perceiving gender as a disadvantage for leadership or research were identified as independent predictors of GBM.
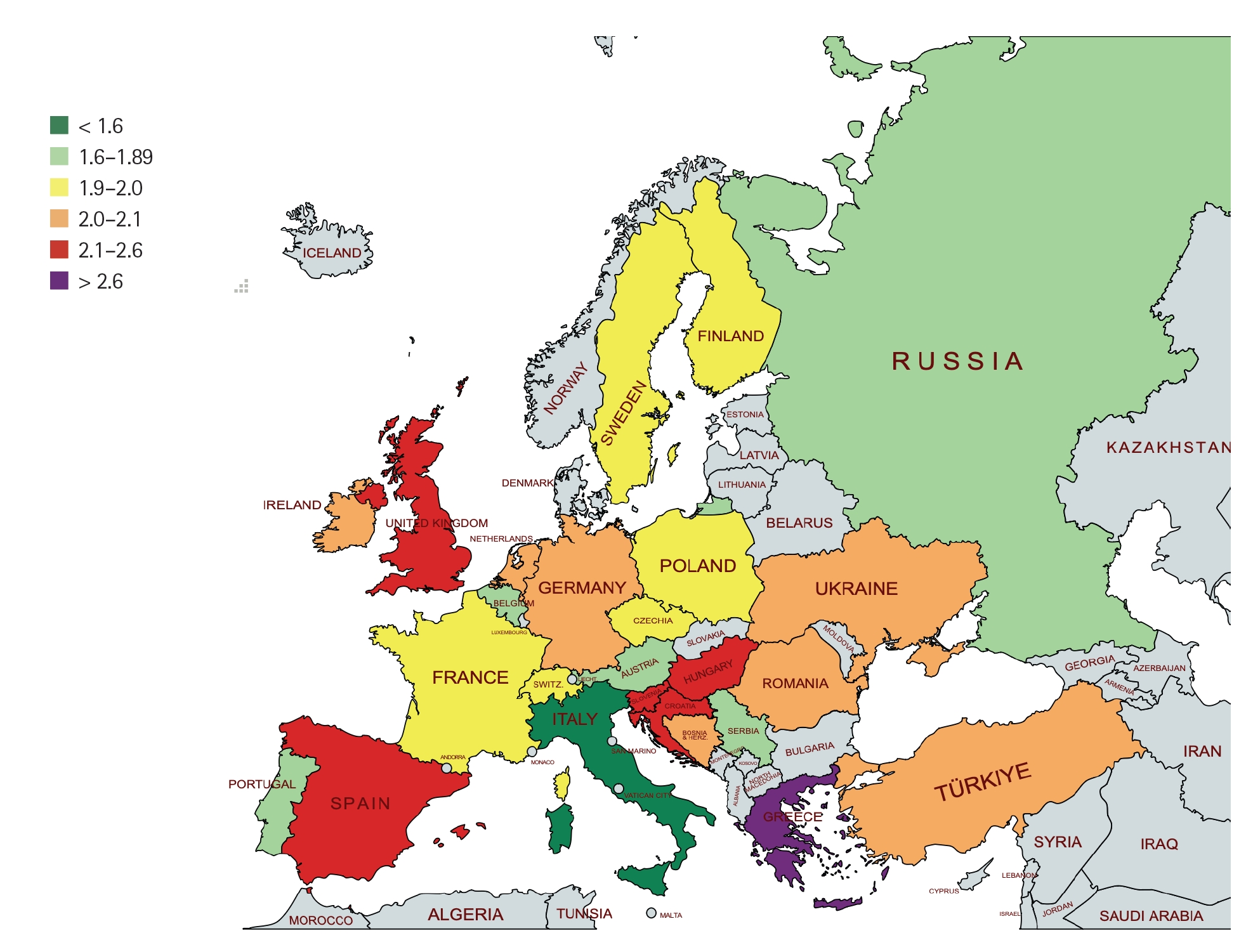
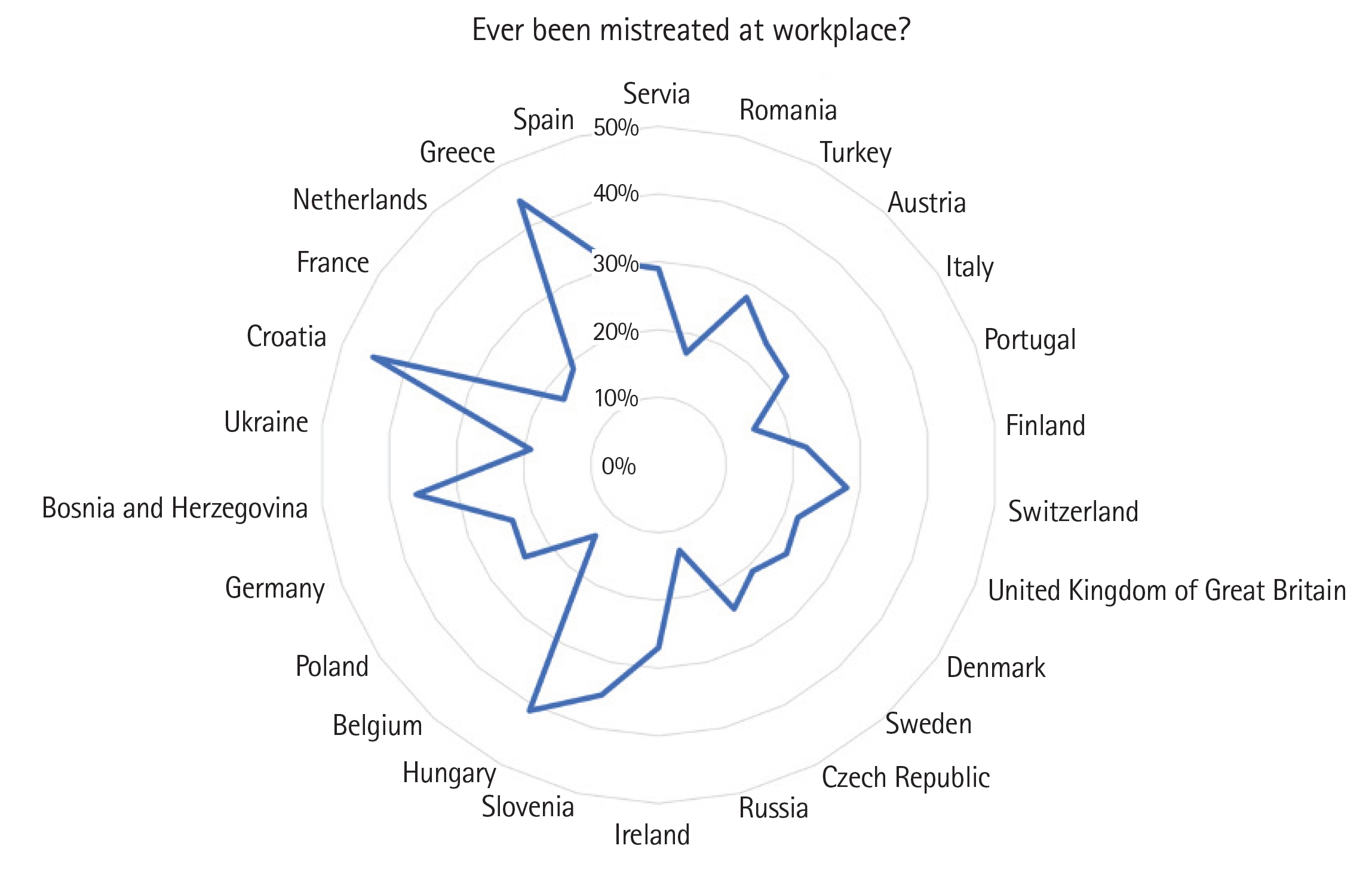
We employed GLMMs to further explore variations in GBM across European countries. The GLMMs were constructed using a binomial distribution and logit link function suitable for the binary nature of the response variable (presence or absence of GBM). Our chosen GLMM incorporated four fixed-effect predictor variables: gender, ratio of women to men in the workplace, gender of the department head, and perception of gender as a disadvantage for leadership. The random effect was the country of practice. This analysis allowed us to rank European countries based on GLMMs and generate the 2020 European GBM Rank in Anesthesiology (Fig. 1, Table 2). Fig. 2 shows the observed rates of Workplace GBM across various European countries. These rates visually represent the state of GBM in each country, with lower rates indicating a more favorable workplace environment in terms of mistreatment.
In addition to our primary results, we conducted model validation analyses to assess the predictive performance and reliability of the GLMMs used to predict the GBM scores for each European country. For detailed results and information on model selection, see the Supplemental Digital Contents (Supplementary Tables 1 and 2). These supplementary analyses ensure transparency and provide a comprehensive explanation of the performance of the statistical model.
Discussion
To the best of our knowledge, this is the first study to analyze GBM data among anesthesiology workplaces in Europe. The most significant predictors of GBM in the workplace were female gender, younger age, perceiving gender as a disadvantage for leadership, and perceiving gender as a disadvantage for research. The 2020 EGMRA, which ranks European countries based on GBM, shows a different ranking from well-known gender equity indices for European countries [27–29], where central and northern European countries are usually placed in the top positions.
Given that gender equity is fundamental for developing more collaborative environments, increasing teamwork efficacy [30], and improving patient outcomes [31–34], effective monitoring of gender equity in the field of anesthesiology is essential. We compared the countries’ overall performance in achieving gender equity in anesthesia using a single measure that combines multiple indicators and dimensions into a single standardized value. The GBM score generated from this study may offer insights into overall gender inequality and inequity in the field of anesthesiology at the national level. It can function as a crucial benchmark for gender equity and could be used to chart the evolution of gender equity over time.
The fact that our predictors for GBM were female gender and younger age was not surprising. Female residents are at risk of several forms of GBM [3,7,35] and are more likely than male residents to report experiences of gender-based discrimination and harassment [4,14,36]. Our GBM ranking shows that mistreatment in anesthesiology does not follow general patterns of gender equity, as seen in the Gender Equality Index [27] or the Global Gender Gap Index [37]. These indices consistently show better performance for Scandinavian countries compared to other European countries, and Mediterranean countries frequently perform below the European average. Thus, applying these general indices to the medical workforce may be inappropriate. These indices primarily measure human development while accounting for gender inequity [29] rather than directly addressing specific factors and considerations pertinent to GBM in the context of the workforce in the medical sector.
Additionally, the degree to which women in anesthesiology face inequity today may differ among countries without necessarily implying a cultural or geographical relationship. However, our ranking trend loosely resembles Eurofound’s index of adverse social behaviors for healthcare workers, where Central, Western European, and Scandinavian countries show the highest percentages of workers reporting violence or harassment in the workplace. Eurofound, short for the European Foundation for the Improvement of Living and Working Conditions, is an EU agency that primarily aims to provide research and information on social and work-related issues to support policy development in Europe. In contrast, a smaller proportion of workers reported GBM in half of the Eastern and Southern European countries [36].
In our analysis, Italy was found to have the lowest gender mistreatment among the countries studied. While pinpointing the precise reasons for this distinction requires careful examination, several pertinent factors may have contributed to Italy’s relatively lower index value. First, Italy’s legislative framework and policies regarding GBM and workplace harassment within the medical sector, including anesthesiology, may be more robust and diligently enforced than those in other countries [38]. Robust legal safeguards and effective reporting mechanisms can reduce the incidence of gender mistreatment. Cultural and societal norms also play pivotal roles in shaping workplace dynamics. Italy may have made significant advancements in promoting gender equality and cultivating respectful environments within anesthesiology [39,40]. Furthermore, Italy’s leadership within anesthesiology societies, such as the Società Italiana di Anesthesia Analgesia Rianimazione e Terapia Intensiva (SIAARTI), may have significantly influenced the lower gender mistreatment index among anesthesiologists. The presence of women in influential roles, including as board chairs, can also foster an inclusive and respectful workplace culture [38]. Therefore, effective reporting mechanisms require further consideration. Italy may have established accessible and efficient systems for reporting gender mistreatment incidents within the field of anesthesiology, which can encourage victims to come forward.
Nevertheless, even within specific medical specialties such as anesthesiology, international comparisons of gender mistreatment indices can be complex because of variations in reporting practices and data collection methods. Italy’s lower index may reflect recent improvements in addressing gender mistreatment within anesthesiology, while other countries may still be implementing comprehensive measures, like, for example, the implementation of clear policies, training programs, reporting mechanisms, diversity initiatives, leadership commitment, and research to tackle GBM and discrimination. Although our analysis suggests that Italy exhibits a lower gender mistreatment index within the specialized context of anesthesiology, further in-depth research into the interplay of these factors and a meticulous examination of workplace practices, policies, and cultural attitudes specific to anesthesiology are needed to gain a more nuanced understanding of this phenomenon.
Some evidence suggests that having more women in leadership roles may be associated with less GBM in the workplace, including sexual harassment and discrimination [41–44]. However, this correlation does not necessarily imply causation. Other factors, such as organizational culture and policies, may also play a role in reducing GBM in the workplace.
Overall, many factors contribute to higher levels of gender harassment among healthcare workers in some European countries. These factors include the absence of legal protections, workplace culture and policies, education and training, and societal norms and values [36]. It is difficult to directly compare the GBM of anesthesiologists in Greece, our worst-ranked country, and other European countries, as GBM is influenced by many factors. However, anesthesiologists in Greece may encounter higher GBM levels partly due to the severe economic crisis that occurred the decade before data collection, leading to cuts in healthcare spending and hospital understaffing [45]. The Greek healthcare system has been underfunded for many years, leading to a shortage of resources, such as medical supplies, equipment, and hospital beds [46]. Despite recent legislation by the Greek government [47] creating policies against violence and harassment in the workplace, enforcement mechanisms may still be lacking, making it easier for GBM to occur.
Limitations
Although our secondary analysis provided valuable insights into the rankings of GBM among European countries based on the collected data, the study had some limitations. This study represents a secondary analysis of a pre-existing dataset. Although the primary survey was global in scale, exploring the European subset provides a valuable opportunity to gain region-specific insights. Our logistic regression analysis identified factors linked to GBM within the European context. It is important to note that this focus on Europe entailed a reduction in sample size, which is acknowledged as a tradeoff. We also acknowledge that gender inequity is multifaceted and thus is often measured using multiple indicators. While gender equity in anesthesia must be effectively monitored, specific dimensions of GBM may also require qualitative assessments. This recognition acknowledges the multifaceted nature of gender equity and the need for subjective experiences and qualitative aspects to be captured that cannot be easily measured numerically. Therefore, combining quantitative and qualitative assessments would provide a more holistic understanding of gender equity in anesthesia and help in addressing the diverse factors that contribute to gender disparities. Additionally, we only examined gender, thus other protected characteristics (e.g., ethnicity, sexual orientation, disability) that should be considered for a more comprehensive understanding of GBM were not assessed. For instance, the observation that women from Low- and Middle-Income Countries appear more ‘content’ than those from Upper Income Countries, as mentioned in our recent paper [14], warrants further investigation to identify the specific factors that contribute to these sentiments.
Efforts to reduce GBM within healthcare, particularly in fields such as anesthesiology, can benefit significantly from data-supported actions. These actions involve harnessing data to inform and implement strategies. Robust data collection and analyses help clarify the prevalence and patterns of GBM and identify areas that require attention [14]. Grounded in data-guided insights, educational programs and awareness campaigns can promote respectful behavior among healthcare professionals and raise awareness about GBM. Data-guided policymaking ensures the development and enforcement of effective anti-GBM measures. In addition, training programs, diverse leadership initiatives, and support for victims can be tailored to data-derived needs [12]. Conducting observations, evaluations, and ongoing research has further enhanced these efforts. International collaboration in sharing data and best practices widens the impact and creates safer and more equitable healthcare environments [48].
Although our study provides valuable insights into the prevalence of GBM among anesthesiologists across Europe, certain limitations must be acknowledged. We recognize that the number of respondents varied according to country, which could have introduced bias into our findings. However, we took steps to address this issue. First, we restricted our analysis to countries meeting specific criteria, including a minimum number of responses (either five per million population or 10% of the members of the national anesthesiologists’ associations). Second, for robust statistical analysis, we required a minimum of 50 respondents per country. Another limitation was the lack of essential demographic and sociodemographic factors in our study such as race, sexual orientation, and disability, all of which could influence how individuals perceive and experience GBM. However, collecting more detailed demographic information may have raised ethical concerns and affected respondents’ willingness to participate. Furthermore, the GBM scores obtained in this study represent only a snapshot assessment of the second half of 2019. Nevertheless, the key aspects of the GBM explored in our analysis can serve as a foundation for future research to track trends in this area over time. In addition, the survey responses could have been affected by subjective judgments. The limitations of our previous study [14] regarding the potential for bias and subjectivity in respondents’ answers also apply to this dataset. We also recognize that the reported rates of GBM may not accurately reflect the true prevalence in each country. Some healthcare workers may choose not to report GBM because of fear of retaliation or job loss. Additionally, some hospitals or healthcare settings may have a culture of tolerance towards GBM or the expectation that healthcare workers should endure mistreatment as part of their job. Such analyses usually benefit from external validation, which was not possible in this study; the data are only from Europe and may not be generalizable to other parts of the world. It is also important to clarify that our intention was not to make broad generalizations based on a single example. Although collecting additional direct information or conducting further surveys involving Italian respondents could have resulted in a more comprehensive understanding, such extensive investigations were beyond the scope of this study. Moreover, providing explanations of our findings may be challenging because data on GBM in anesthesia and other fields are limited in most European countries. Finally, although the original survey included a non-binary gender option, only a small proportion of participants identified as non-binary; therefore, further statistical analyses were precluded. These limitations underscore the need for ongoing research efforts to offer a more holistic understanding of GBM in the context of anesthesiology across Europe. Incorporating nuanced analyses that consider contextual factors, such as national policies, institutional dynamics, and healthcare system structures, is essential for understanding the complexities of GBM across different countries. Further examinations of cases in Italy, where potential preferential treatment policies exist, could provide valuable insights into how these factors intersect with the anesthesiologists’ experiences of GBM.
Scientific and institutional interest in workplace inequity is rapidly increasing. Therefore, our methodologically-validated ranking could be used as a monitoring tool. However, specific intrapersonal, interpersonal, or socio-environmental factors are often used as an inaccurate explanation for the cause of GBM. Our ranking aims not only to provide initial insight into GBM among anesthesiologists in Europe, but also to function as a key benchmark for gender equity and to chart the evolution of disparities over time.