Introduction
Epidural analgesia is considered the gold standard for labor analgesia. Although provider-administered manual epidural infusion is classically performed as labor analgesia, with advances in technology, new methods, such as continuous epidural infusion and programmed intermittent epidural bolus (PIEB), have been introduced. Both are widely used in clinical situations for labor analgesia in combination with an epidural bolus [1].
PIEB is a method of automatically injecting a local anesthetic into the epidural space [2]. It provides superior analgesia and decreases motor blockade compared with conventional continuous epidural infusion [3]. PIEB is known to have an effective analgesic effect because it distributes the local anesthetic more uniformly in the epidural space with a large volume and high flow rate [4]. However, no standard for the appropriate flow range of PIEB has been established to date. Although Klumpner et al. [5] have reported that the higher the infusion rate, the higher the pressure generated during PIEB, Lange et al. [6] demonstrated that a small difference in epidural infusion flow rates (100 ml/h vs. 300 ml/h) did not contribute to satisfactory labor analgesia. Furthermore, because providing a high flow rate above a certain level is difficult owing to the pressure limitations of the machine itself, additional research is needed to establish a satisfactory epidural infusion flow rate.
Based on this, we hypothesized that a high-flow epidural bolus infusion of local anesthetics would be more efficient than a low-flow bolus infusion during labor analgesia. Therefore, we aimed to compare the effects of epidural analgesics infused at different flow rates on labor analgesia.
Materials and Methods
Ethics
This randomized, parallel-group, single-blind study was approved by the Institutional Review Board of Samsung Medical Center, Seoul, Republic of Korea (No. SMC 2019-06-085-002, chairperson Young Keun On, registration date: 11/09/2019) and was registered in the Clinical Trial Registry of Korea (https://cris.nih.go.kr, registration no. KCT0004389, principal investigator: Duck Hwan Choi, date of registration: 28/10/2019) a written informed consent was obtained from all participants before study enrolment. All the procedures were performed in accordance with the Declaration of Helsinki, 2013.
Patients
The study was conducted between November 2019 and December 2020. Nulliparous women with gestational age ≥ 36 weeks, single-tone pregnancy, American Society of Anesthesiologists physical status of I or II scheduled for spontaneous or induced vaginal delivery with cervical dilatation between 2 and 5 cm, and regular contractions occurring every 3–5 min were included. The exclusion criteria were as follows: women who received opioids or sedatives, received opioids within 4 h prior to labor analgesia, hypersensitivity, allergy to local ropivacaine or fentanyl, preeclampsia, and premature rupture of membranes.
Randomization and blindness
One statistician who was not involved in this study generated a random allocation sequence. Participants were randomly assigned to one of the three study groups using a computer-generated randomization sequence: continuous, PIEB, or manual. Randomization and group allocation were performed in a 1:1:1 ratio with a block size of three. One of the authors assigned the groups using the sealed opaque envelope technique. All investigators were blinded to the assigned groups.
Study protocol
A combined spinal epidural analgesia (CSE) procedure for labor analgesia was performed by residents under the supervision of an experienced obstetrical anesthesiologist. Prior to the procedure, the patient’s intravenous route was secured, and standard monitoring was performed, including blood pressure, heart rate, pulse oximetry, respiration rate, fetal heart rate, and uterine contractions. At the L3–4 interspace with the patient in the lateral decubitus position, a lumbar puncture was performed using a 25-gauge Whitacre needle (BD® Whitacre spinal needle, 25 G × 3.50IN TW, BD). After confirming the free flow of cerebrospinal fluid, intrathecal agents (0.2% ropivacaine 3 mg with fentanyl 20 μg) were administered to relieve labor pain immediately. The epidural space was then located using a 17-gauge Tuohy needle at the L3–4 or L4–5 level with the loss of resistance to the air technique. An epidural catheter (FlexTip Plus® Epidural Catheterization Set, 19 G, Arrow Electronics) was inserted 5–6 cm into the epidural space, confirmed by negative aspiration of blood and cerebrospinal fluid and flushed with 4 mg of 0.2% ropivacaine. All the procedures were performed using aseptic techniques.
According to the assigned group, an ambulatory infusion pump (Accumate® 1200, Wooyoung Meditech Co., Ltd.), comprising 60 ml of 0.2% ropivacaine, fentanyl 180 μg, and 40 ml of 0.9% saline, was used. Prior to the start of this trial, an ambulatory infusion pump device was tested using an infusion device analyzer (IDA-4 Plus Multi-Channel Infusion Device Analyzer, Fluke® Biomedical) to confirm its applicability. Patient-controlled epidural analgesia (PCEA) was prepared by a nurse who was not involved in the trial.
The details of drug delivery protocol according to the assigned group were as follows. In the continuous group, PCEA + basal continuous epidural infusion 10 ml/h was started 30 min after the labor analgesia procedure. When the bolus button was pressed by the patient, 5 ml of the local anesthetic was injected. Continuous basal epidural infusion was continued, regardless of the bolus dose.
In the PIEB group, PCEA + PIEB 10 ml during one hour (240 ml/h for bolus infusion of 10 ml) and infusion were started 60 min after the labor analgesia procedure. When the bolus button was pressed by the patient, 5 ml of local anesthetic was injected and a PIEB was injected after 15 min.
In the manual group, PCEA + provider-administered intermittent epidural boluses of 10 ml during one hour (1,200 ml/h for bolus injection of 10 ml) and manual injection was started 60 min after the labor analgesia procedure. In the manual group, an experienced anesthesiologist injected 10 ml of ropivacaine with a fentanyl mixture at a constant rate for 30 s through an epidural catheter. When the bolus button was pressed by the patient, 5 ml of the local anesthetic was injected. A provider-administered epidural bolus was injected at set intervals regardless of the bolus dose.
Labor pain was measured using an 11-point numerical rating scale (NRS: 0 = no pain and 10 = the worst pain imaginable). The participants were informed that the PCEA bolus could be used for labor analgesia. Breakthrough pain was defined as pain requiring a bolus infusion of PCEA while receiving epidural anesthetics according to the assigned group. When breakthrough pain with an NRS score ≥ 4 occurred during PCEA infusion, rescue medications were injected as follows: 0.2% ropivacaine 14 mg was administered into the epidural space. If the pain did not subside, 50 mg of 1% lidocaine was administered. The delivery method was switched from vaginal delivery to Cesarean section in cases where failure to progress in labor occurred even after more than 4 h of labor or when the mother requested it.
Patients’ age, height, weight, body mass index, gestational age, cervical dilatation at the time of labor analgesia, total labor duration, any adverse effects associated with labor analgesia (e.g., nausea, vomiting, numbness, paraplegia, postdural puncture headache, and local anesthetic systemic toxicity), duration of second stage, incidence and NRS score of breakthrough pain, use of oxytocin, preoperative blood pressure, heart rate, NRS score after the labor analgesia procedure, conversion rate to Cesarean section, and patient satisfaction using a Likert scale were also recorded.
Outcomes
The primary outcome was the hourly consumption of epidural analgesics during the labor analgesia procedure among the three groups. The secondary outcomes were the differences in the time interval to the first breakthrough pain, NRS score for breakthrough pain, degree of sensory and motor nerve blockade, and NRS score 4 h after labor analgesia among the three study groups. Considering the duration of intrathecal anesthetics injected during the labor analgesia procedure, we investigated the degree of sensory and motor blockade 4 h after the labor analgesia procedure. Neonatal outcomes including birth weight and Apgar scores were also recorded.
The degree of sensory blockade was recorded using a cold sensation, and the degree of motor blockade was investigated using the Breen-modified Bromage score (1 = complete block, unable to move feet or knees; 2 = almost complete block, only able to move feet; 3 = partial block, only able to move below knees; 4 = detectable weakness of hip flexion while supine; 5 = no detectable weakness of hip flexion while in supine but cannot stand due to hip weakness, full flexion of knees; and 6 = can stand and perform partial knee bend) [7].
Statistical analyses
A power calculation was based on a previous study that investigated the effect of PCEA plus automated mandatory boluses (PIEB) for reducing the hourly consumption of local anesthetics during labor (mean ± standard deviation [SD]: control group, 7.5 ± 2.0 ml vs. PIEB group, 6.5 ± 3.4 ml) [8]. We hypothesized that the difference in hourly local anesthetic consumption among the three groups would be clinically significant at a minimum of 1 ml. Thus, we calculated that 28 patients per group would provide a power of 80% at a significance level of 5%, under the assumption that the difference in local anesthetic consumption among the three groups was clinically significant. Considering a dropout rate of 10%, a minimum of 31 patients in each group (n = 93) were required to participate in the study.
Continuous variables are expressed as mean ± SD, median (Q1, Q3), or median (min, max) while normality was assessed using the Shapiro–Wilk test. For motor blockade and NRS score 4 hours after labor analgesia induction, the min and max values were additionally described. Categorical variables are expressed as numbers (percentages). A one-way analysis of variance or Kruskal–Wallis test was used as appropriate to determine the differences in continuous variables among the study groups, including hourly consumption of epidural analgesics, time interval to the first breakthrough pain, NRS score for breakthrough pain after labor analgesia, degree of sensory and motor nerve blockade, NRS score at 4 h after the labor analgesia procedure, and obstetric and neonatal outcomes. In case of statistical differences among the three groups, multiple comparisons were performed using Bonferroni correction. Categorical variables, including the incidence of breakthrough pain and mode of delivery, were analyzed using Pearson’s chi-square test. The partitioned chi-square test was used for multiple pairwise comparisons. Bonferroni correction was used to adjust P values for multiple comparisons. Statistical analyses were performed using SPSS® version 25 (IBM® Inc.), and P < 0.05 was considered significant.
Results
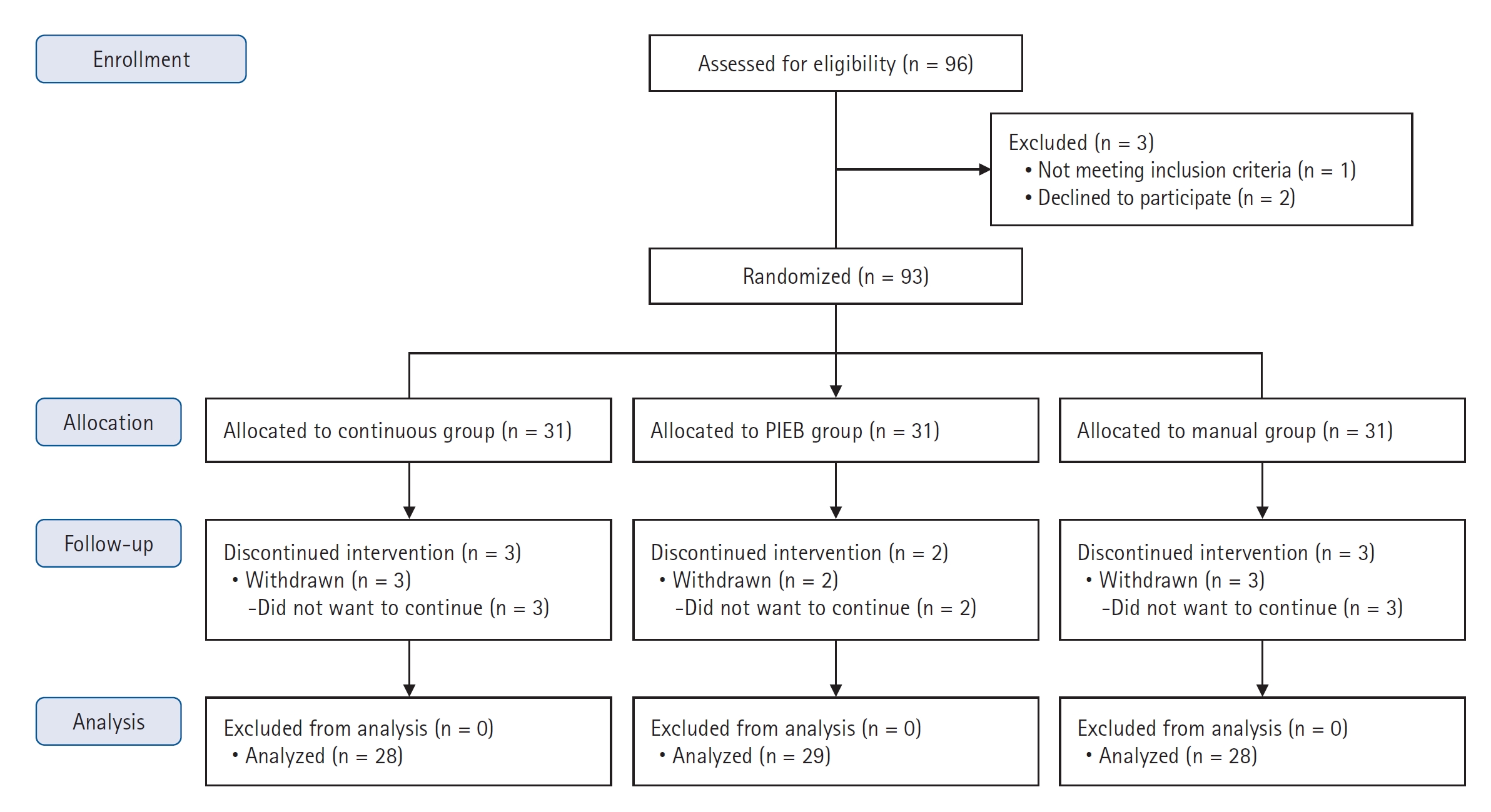
Altogether, 96 parturient women were examined for eligibility, and three were excluded for not meeting the inclusion criteria (n = 1) and declining to participate (n = 2). Additionally, eight women withdrew from the trial because they did not want to continue participating. Finally, 85 participants completed the trial as follows: continuous group (n = 28), PIEB group (n = 29), and manual group (n = 28) (Fig. 1). When labor analgesia was administered, no difference in cervical dilation was observed among the three study groups (continuous: 3 [3, 3] cm, PIEB: 3 [3, 3] cm, manual: 3 [3, 3] cm), respectively; all the participants received oxytocin. The NRS scores before labor analgesia were comparable in all three groups (continuous: 6 [5, 8], PIEB: 6 [5, 7], manual: 5 [5, 6]). The demographic data were similar between the study groups (Table 1).
No differences in the duration of PCEA application were observed among the three groups (P = 0.285) (Table 2). However, the hourly consumption of epidural analgesics was significantly different among the three study groups (continuous: 14.3 [4.7, 12.9] ml, PIEB: 9.4 [6.2, 9.8] ml, manual: 8.6 [7.6, 9.9] ml; P < 0.001). Moreover, significant differences in the hourly consumption of epidural analgesics were observed between the continuous group and the other groups (continuous vs. PIEB, P < 0.001; PIEB vs. manual, P = 0.413; and continuous vs. manual, P < 0.001) (Fig. 2).
Participants requiring PCEA bolus infusion due to breakthrough pain were 22 (78.9%) in the continuous group, 19 (65.5%) in the PIEB group, and 14 (50.0%) in the manual group (P = 0.081). The NRS scores at the time of complaining of breakthrough pain were not significant among the three groups (continuous: 4.0 [0.2], PIEB: 4.0 [1.0], and manual: 3.5 [1.0], P = 0.195). The PIEB group expressed breakthrough pain after a significantly longer time than the manual group (continuous: 78.5 [35.8, 185.0] min, PIEB: 200.0 [88.5, 441.5] min, manual: 60.5 [37.3, 162.0] min; P = 0.027) (Table 2).
No significant differences in the degree of sensory and motor blockade were observed among the study groups 4 h after labor analgesia induction (sensory blockade, P = 0.974; motor blockade, P = 0.224). Two cases of motor nerve blockage were recorded 4 h after infusion: one each in the continuous and manual groups. The NRS scores were not significantly different among the three groups 4 h after labor analgesia induction (P = 0.066). Obstetric and neonatal outcomes are presented in Table 3. A significant difference in the mode of delivery was observed among the three groups (continuous: 18 [64%], PIEB: 27 [93%], and manual: 18 [64%], P = 0.021). In pairwise comparisons, the mode of delivery did not indicate a significant difference according to the epidural injection method (continuous vs. PIEB, P = 0.069; PIEB vs. manual, P = 0.081; manual vs. continuous, P > 0.99). Although three participants complained of numbness in the lower extremities immediately after labor analgesia induction, they recovered within 4 h. Two participants in the continuous group required 14 mg of 0.2% ropivacaine as an epidural rescue medication. No adverse events occurred during the study period.
Discussion
This randomized clinical trial demonstrated that PIEB or manual infusion of epidural analgesics effectively reduced the hourly consumption of epidural analgesics rather than continuous epidural infusion in labor analgesia. Moreover, the time taken to express the first breakthrough pain after labor analgesia induction was significantly longer in the PIEB group than in the other groups.
Numerous studies have demonstrated that intermittent epidural bolus injection provides superior labor analgesic effects compared with continuous infusion, reducing local anesthetic consumption and increasing maternal satisfaction [8–13]. A systematic review has indicated that larger bolus doses of diluted epidural anesthetics are required for superior analgesia [14]. In this context, Wong et al. [15] demonstrated that administration of larger doses of epidural anesthetics at long time intervals reduces the consumption of bupivacaine and increases maternal satisfaction (2.5 ml/15 min vs. 5 ml/30 min vs. 10 ml/60 min). Most previous studies on PIEB compared bolus volumes and time intervals. However, studies comparing differences in the flow rate of administered drugs are lacking.
Lange et al. [6] who investigated the difference in the effect of the PIEB according to the flow rate (100 ml/h vs. 300 ml/h), have reported that the hourly consumption of epidural analgesics was not improved by high-flow epidural administration. In line with this, our results revealed no significant difference in epidural analgesic consumption between the PIEB and manual injections. As our study and that of Lange et al. differed slightly because Lange et al. [6] conducted a study using only the PIEB machine, the difference in infusion pressure between the groups might not be significant. Considering that analgesic consumption may be related to the flow rate of epidural analgesics, we provided a higher infusion flow rate (1,200 ml/h) via manual injection. Additionally, the flow rate of the PIEB group was selected as the maximum value that could be set in the machine (240 ml/h). Hence, the flow rate in the PIEB group was sufficient to provide effective labor analgesia compared with the high flow rate in the manual group. In Lange et al.’s study, the authors suggested that several factors may affect these results, including the size of the epidural catheter, number of orifices, dose and concentration of the local anesthetic, and infusion rate of the bolus drug. To exclude the influence of external circumstances, we equally administered epidural analgesics, epidural catheters, and PCEA machines to each group in this study. Consequently, the flow rate of the epidural bolus injection for adequate labor analgesia may not need to be excessively high. Effective labor analgesia can be provided within the range of the flow rate provided by the machine.
PIEB has a superior analgesic effect compared to continuous infusion because the drugs are distributed at high pressures in the epidural space and effectively block sensory nerves. Because most PCEA machines allow the limit of high rates as 200–300 ml/h, this is insufficient to assess the effectiveness of high-flow vs. low-flow epidural infusion. We expected that manual infusion would increase the diffusion range by promoting better drug flow within the epidural space. However, our findings demonstrated that the labor analgesic effect of manual injection was not different from that of PIEB. Although this study did not establish the flow rate range that can provide optimal labor analgesic effects, the infusion flow rate into the epidural space did not need to be as high as that of manual infusion. Therefore, parous women may likely achieve sufficient analgesic effects with the PIEB machine.
Intermittent boluses are associated with a greater diffusion surface area than continuous infusions [16]. Thus, local anesthetics do not remain in a specific epidural space for a long time and are distributed in a large space at a fast rate during PIEB. By contrast, because the concentration of local anesthetics is more easily elevated in the extraneural space than in the intraneural space during continuous infusion, motor blockade frequently occurs [3,17]. Preserving the motor function during labor analgesia maintains the pelvic muscle tone. This enables smooth pushing during the delivery process and reduces the transition to instrumental delivery. Although numerous studies have compared motor blockade according to the epidural injection method, the results have been inconsistent. Capogna et al. [3] have demonstrated that the incidence of motor blockade was lower with PIEB than with continuous infusion. Meanwhile, no significant difference in the degree of motor blockade was observed between the PIEB and continuous infusion in this study. This discrepancy may be related to the type of local anesthetic used. Previous studies using similar concentrations of ropivacaine as ours did not demonstrate a difference in the incidence of motor blockade between continuous epidural analgesia and PIEB [8,11,18]. These evidences support the involvement of the type and concentration of local anesthetic in the incidence of motor blockade. When selecting a labor analgesic regimen using epidural analgesia, applying it in clinical practice would be desirable, considering that the use of a low concentration and large volume of local anesthetic promotes effective labor analgesia without motor blockade [19].
As mentioned above, no significant difference in the incidence of motor blockade was observed regardless of the method of epidural infusion of the local anesthetic used in this study. However, the rate of conversion to Cesarean section was significantly lower in the PIEB group. Our results contradict those of Huang et al. [20], who have reported no difference in the conversion rate of the mode of delivery between PIEB and continuous infusion. In particular, no significant difference in the mode of delivery conversion rate according to the epidural infusion method was indicated in studies using the same local anesthetic at a concentration similar to this study [8,11,21]. Since we used low and high doses of the local anesthetic in this study, the local anesthetic could have been more effectively distributed in the epidural space in the PIEB group than in the other groups. By contrast, a higher dose of local anesthetic could have been distributed in the extraneural space in the continuous-infusion group. A previous meta-analysis investigating the rate of assisted vaginal delivery according to the concentration of local anesthetics (high vs. low) supports our suggestion [22].
This study has several limitations. First, we used the CSE method rather than the simple epidural analgesia as the labor analgesia method, and the same intrathecal agent was administered to all the participants. Thus, the outcomes of our study may have been affected by the extended duration and range of the intrathecal drugs. However, the duration of intrathecal ropivacaine administration was less than 100 min [23]. Considering that all groups in our study applied PCEA for more than 390 min, the effects of intrathecal agents would disappear when our secondary outcome was measured. Second, different results may have been obtained depending on the specifications of the PCEA machine used at each institute. Third, each local anesthetic used for labor analgesia has a different viscosity [24]. Future studies are required to investigate the effects of different PCEA machines and local anesthetics on the flow rate and infusion pressure generated when the local anesthetic is distributed into the epidural space. Finally, the infusion flow rate might not have been constant in the manual group. The epidural space is a potential space where the pressure and volume of the injected medication can affect the distribution of agents. Therefore, the pressure generated by the infusion of epidural agents may have individual differences that may have influenced the study outcomes. However, these effects occurred not only in the manual group, but also in the other two groups. Considering that the study design was a randomized trial, the influence of the epidural space may be evenly distributed among all the participants.
In conclusion, PIEB with ropivacaine provided adequate analgesia and did not require the high flow provided by manual injection for labor analgesia. Future research is warranted to determine the ideal flow rate of PIEB.