Introduction
Perioperative blood pressure management is essential for anesthesiologists and intensivists because intra- and postoperative hypotension is associated with myocardial injury, acute kidney injury, and mortality [1ŌĆō6]. In the noncardiac surgery setting, blood pressure management strategies are often used to optimize perioperative blood pressure [7,8]. However, catecholamines such as norepinephrine and dopamine are normally initiated when fluid administration fails to restore adequate arterial blood pressure and organ perfusion, which may affect mortality and morbidity [9].
Norepinephrine is a potent alpha-1 and beta-1 adrenergic receptor agonist that induces vasoconstriction and increases mean blood pressure [10]. In septic shock, a greater improvement in mortality has been found with norepinephrine than with dopamine [10ŌĆō13]. Norepinephrine has also been associated with lower in-hospital and intensive care unit (ICU) mortality compared with dopamine in a population of patients, 60% of which had cardiac disease or were post-cardiac surgery [14]. Additionally, a subgroup analysis of a randomized controlled trial showed a greater decrease in mortality with norepinephrine than with dopamine in cardiogenic shock but no difference was observed in hypovolemic shock [12]. These previous studies comparing norepinephrine and dopamine have investigated post-cardiac surgery and septic patients, and based on this, physicians have selected perioperative vasoconstrictors [15]. However, studies comparing the effects of norepinephrine and dopamine in noncardiac surgery settings with relatively low mortality are limited [9].
In the present study, we hypothesized that a greater improvement in mortality is found with norepinephrine than with dopamine in patients after noncardiac surgery. Therefore, we aimed to evaluate the effects of postoperative norepinephrine and dopamine on clinical outcomes in adult patients after noncardiac surgery by analyzing a nationwide intensive care patient database.
Materials and Methods
Ethical statement
This study was approved by the Ethics Review Board of the Hamamatsu University School of Medicine (approval number 22-025) and the Japanese Intensive care PAtient Database (JIPAD) working group. The requirement for informed consent was waived because of the anonymity of the data. This study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines [16].
Data source
We conducted this multicenter retrospective study using the JIPAD, which has been managed by the Japanese Society of Intensive Care Medicine since 2014 [17]. At the time of this study (May 2022), data on 184,705 individuals from 70 facilities were collected. The JIPAD aims to adhere to global standards and shares common codes with the Australian and New Zealand Intensive Care Society Adult Patient Database (ANZICS-APD) and the Intensive Care National Audit & Research Centre Case Mix Program (ICNARC-CMP). Anonymized data are collected and submitted to the JIPAD by physicians involved in daily patient care that ranges from diagnoses, routes of admission, and vital signs to treatment details, complications, and discharge outcomes. To maintain data accuracy, physicians responsible for data management at each participating facility undergo training on the query system, which is a program used to check the validity and reliability of the input data [17]. The JIPAD working group checks the registration data and provides feedback on the data quality in each ICU several times per year. For clinical research, the JIPAD working group approves research protocols and distributes the anonymized data.
Patient selection
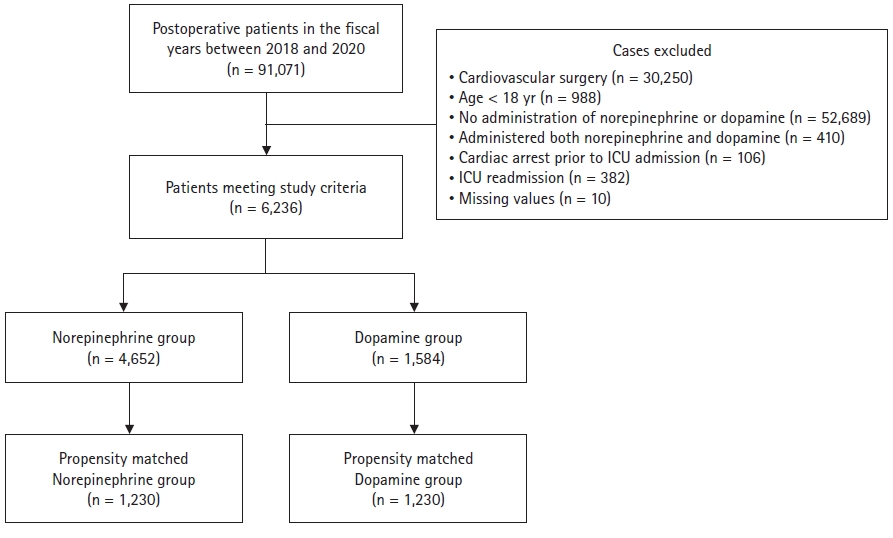
As catecholamine data were not collected in the JIPAD until 2017, this study analyzed the JIPAD data from the fiscal years 2018 to 2020. The inclusion criteria consisted of the following: 1) ICU admission after surgery, 2) age > 18 yr, and 3) administration of either norepinephrine or dopamine within 24 hours of ICU admission. The exclusion criteria were as follows: 1) diagnostic code for cardiovascular surgery, 2) age < 18 yr, 3) no administration of norepinephrine or dopamine, 4) administration of both norepinephrine and dopamine, 5) cardiac arrest before ICU admission, 6) readmission to the ICU, and 7) missing data.
Exposure and outcomes
Patients were divided into the norepinephrine and dopamine groups based on the drugs administered within 24 h of ICU admission. In the JIPAD, norepinephrine and dopamine are registered in categories based on maximum dosages within 24 h. Norepinephrine was classified into low (Ōēż 0.1 ┬Ąg/kg/min) and high (> 0.1 ┬Ąg/kg/min) dosages, and dopamine was classified into low (Ōēż 5 ┬Ąg/kg/min), medium (> 5 to Ōēż 15 ┬Ąg/kg/min), and high (> 15 ┬Ąg/kg/min) dosages [14]. The primary outcome was in-hospital mortality. Secondary outcomes were ICU mortality, hospital length of stay, and ICU length of stay.
Variables
The following variables were collected from the JIPAD: facility identification number, fiscal year of admission, age, sex, weight, height, ICU/hospital length of stay, chronic comorbidities (congestive heart failure, respiratory failure, liver failure, cirrhosis, use of immunosuppressants, hemodialysis, lymphoma, acute leukemia, and cancer with metastasis), planned ICU admission (or emergency ICU admission), planned surgery (or emergency surgery), diagnostic codes, Acute Physiologic and Chronic Health Evaluation III (APACHE III) score, Japan Risk of Death (JROD) score, APACHE II score, Simplified Acute Physiology Score II (SAPS II) score, Sequential Organ Failure Assessment (SOFA) score, post-tracheotomy at ICU admission, invasive blood pressure monitoring, central venous catheter use, mechanical ventilation, acute kidney injury, dobutamine use, and epinephrine use. The body mass index was calculated and categorized according to the World Health Organization definitions. The types of surgery were classified into seven categories: respiratory, gastrointestinal, neurological, trauma, urological/genitourinary, obstetrical/gynecological, and musculocutaneous, in accordance with the JIPAD diagnostic codes. Surgery for infection control was defined in accordance with the JIPAD dictionary. The JROD is a more accurate predictor of mortality and ensures better adjustment for case-mix variation than the APACHE III [18].
Statistical analysis
We used propensity score analysis to adjust the baseline characteristics between the norepinephrine and dopamine groups. To calculate propensity scores, a generalized estimating equation model with clustering according to the participating facilities was applied. The following variables were used in the model: fiscal year at ICU admission, age, sex, body mass index category, chronic comorbidities, planned ICU admission, planned surgery, surgical categories, surgery for infection control, APACHE III score, JROD score, APACHE II score, SAPS II score, SOFA score, post-tracheotomy on ICU admission, invasive blood pressure monitoring, central venous catheter use, mechanical ventilation, acute kidney injury, dobutamine use, and epinephrine use. We performed one-to-one nearest-neighbor matching without replacement for the estimated propensity scores using a caliper width set at 20% of the standard deviation of the propensity scores on the logit scale [19,20]. For each variable, balances in baseline variables using absolute standardized differences were examined, and values < 10% were considered balanced [21]. Categorical variables were reported as numbers and percentages, and continuous variables were reported as medians and interquartile ranges (IQRs). We described the maximum dosage of norepinephrine and dopamine within 24 h of ICU admission.
We calculated the risk differences and 95% CIs for in-hospital mortality after propensity score matching. Chi-square tests were used for comparisons between the two groups. In terms of the secondary outcomes, ICU mortality was evaluated using the same analytical method used for the primary outcome, while the median and IQR were calculated for the continuous data (hospital and ICU length of stay). The Wilcoxon rank-sum test was used to compare the two groups. Two-sided P values < 0.05 were considered statistically significant. All analyses were performed using Stata/BE 17 software (STATA Corp., USA).
Results
After applying the inclusion and exclusion criteria, we identified 6,236 patients from 69 facilities (Fig. 1). The patients were divided into the norepinephrine (n = 4,652) and dopamine (n = 1,584) groups. One-to-one propensity score matching resulted in 1,230 pairs. The c-statistic of the propensity score model was 0.82.
Table 1 shows baseline patient characteristics before and after propensity score matching. Patients were more likely to receive norepinephrine if they were registered in 2020; had congestive heart failure; underwent gastrointestinal, trauma, gynecological, or musculocutaneous surgery; underwent surgery for infection control; had a high APACHE III, JROD, APACHE II, SAPS II, or SOFA score; required a central venous catheter; underwent mechanical ventilation; had acute kidney injury; or were administered dobutamine or epinephrine. Patients were less likely to receive norepinephrine if they were registered in 2018, male, of normal weight, received immunosuppressants, had a planned ICU admission, underwent planned surgery, underwent respiratory or renal/genitourinary surgery, or were post-tracheotomy at ICU admission. After propensity score matching, the patient characteristics were well balanced between the two groups.
Fig. 2 illustrates the maximum catecholamine dosage categories. The low-dose category was the most common in both groups, with 1,003 (81.5%) patients in the norepinephrine group and 1,056 (85.9%) in the dopamine group.
Table 2 shows all outcomes after propensity score matching. In-hospital mortality did not differ between the two groups overall (norepinephrine vs. dopamine: 4.2% vs. 3.8%; risk difference: 0.41%, 95% CI [ŌłÆ1.15, 1.96], P = 0.608). For the secondary outcomes, ICU mortality and hospital length of stay did not differ significantly between the groups. In contrast, ICU length of stay was significantly shorter in the norepinephrine group compared with the dopamine group, with a median ICU stay of 3 days in the norepinephrine group and 4 days in the dopamine group (P < 0.001).
Discussion
In this analysis of nationwide intensive care data on 6,236 patients from 91,071 adult postoperative patients, we compared the effectiveness of norepinephrine and dopamine in patients after noncardiac surgery. No significant difference in in-hospital mortality was observed between the two groups. Although the median ICU length of stay in the norepinephrine group was approximately one day shorter than that in the dopamine group, ICU mortality and hospital length of stay did not differ significantly between the groups.
Our findings were consistent with those from a Cochrane review that reported no evidence that norepinephrine was more effective at reducing mortality than dopamine [22]. In contrast, norepinephrine has been reported to reduce mortality more than dopamine in cardiogenic and septic shock [12ŌĆō14]. Three potential explanations for this inconsistency are discussed here. First, the mortality rate of eligible patients in this study differed from that reported in previous studies. In-hospital mortality was 4.2% in the norepinephrine group in this study, while previous studies have reported ranges from 17.4% to 56.6% [12,14], suggesting that norepinephrine or dopamine use may not be a concern in a population with relatively low mortality. Second, we noted a difference in the catecholamine dosage between this study and previous reports. Catecholamine dosage has been reported to be a significant factor in mortality, with exceptionally high mortality reported for norepinephrine doses Ōēź 1 ┬Ąg/kg/min and dopamine doses Ōēź 15 ┬Ąg/kg/min [14,23]. More than 80% of our patients received a low dosage of norepinephrine or dopamine, suggesting that physicians only used these agents to optimize perioperative blood pressure. Finally, differences in mortality may be due to physiological differences between the various types of shock. After noncardiac surgery, patients are thought to develop hypotension due to hypovolemia [24]. In hypovolemic shock, catecholamine therapy aims to maintain perfusion pressure temporarily until tertiary treatment is completed, which differs from septic shock, which is physiologically vasodilatory [25].
The present study showed that, although the norepinephrine group exhibited a significantly shorter ICU length of stay than the dopamine group, the hospital length of stay did not differ significantly between the groups. Suzuki et al. [14] reported that dopamine was associated with a longer ICU length of stay but not with hospital length of stay in a population among which 60% had cardiac diseases. As numerous reports have shown that norepinephrine is less arrhythmogenic than dopamine in septic and cardiogenic shock, the shorter ICU stay may be attributable to arrhythmia management [10,13,26]. The approximate increase in ICU length of stay by one day associated with the administration of dopamine may provide a rationale for the use of norepinephrine, as extended stays in the ICU may result in a higher incidence of infections and higher medical costs than shorter stays in the ICU [27,28].
Accumulating evidence has indicated that norepinephrine can be safely administered through peripheral venous catheters [10,29], and various studies on perioperative norepinephrine use have been conducted [30ŌĆō33]. However, our findings indicate that norepinephrine may not have a greater effect on mortality than dopamine in the noncardiac postoperative setting in populations with relatively low expected mortality rates. Our results indicate that, in terms of blood pressure optimization in noncardiac surgery (unlike that in septic or cardiogenic shock), norepinephrine may have a slight advantage over dopamine.
In the present study, the dosages of norepinephrine and dopamine administered were inconsistent. Previous studies have shown that the potency of dopamine is 1/100th that of norepinephrine [34]. Evaluating the low-dose category of the present study (norepinephrine Ōēż 0.1 ┬Ąg/kg/min and dopamine < 5 ┬Ąg/kg/min), which comprised more than 80% of the study population, showed that norepinephrine had a greater potency than dopamine. The subsequent decrease in ICU stay by 1 day, despite the increased potency of norepinephrine relative to dopamine, suggests that norepinephrine might possess a pharmacological advantage over dopamine in the perioperative setting. However, physicians adjust the dosage of catecholamines in accordance with the intended mean arterial pressure. Even if a randomized controlled trial was performed to compare norepinephrine and dopamine, it would be unfeasible to preserve comparable drug potencies.
We acknowledge that this study had a few limitations beyond those typical of retrospective studies. First, catecholamine information registered in the JIPAD is categorized as the maximum dosage within 24 h of ICU admission, with no record of exact catecholamine dosing times, average dosages, or data during surgery or after 24 h. The JIPAD does not contain catecholamine data for the 2015ŌĆō2017 period or information regarding other vasopressors such as vasopressin, phenylephrine, milrinone, or levosimendan. The JIPAD also does not include long-term data (such as 90-day mortality) and organ data, including arrhythmia, neurological sequelae, myocardial ischemia, and ventilator-associated pneumonia. In addition, we could not collect information on the indication for the study drugs (e.g., target mean arterial pressure, mixed venous oxygen saturation, cardiac index, stroke volume variation). Although a nationwide database was used for this study, future prospective studies are needed because data cannot be collected from the JIPAD without registration. Second, several types of selection bias may have been present in this study given the exclusion of patients who received both norepinephrine and dopamine and those with missing values as a propensity score could not be calculated for those patients. However, compared with the 6,236 patients in the overall cohort, the number of patients who received both catecholamines (410) or had missing data (10) was small enough to not have significantly affected the results. Third, although the JIPAD is a newly established ICU registry and the number of facilities registered in the database increases every year, the registry database does not cover all ICUs in Japan. Therefore, the facilities registered in the JIPAD, which are university hospitals or other hospitals with considerable human resources, may not represent the entire cohort in Japan. In addition, the JIPAD is smaller in scale than the ANZICS-APD and ICNARC-CMP databases, leaving room for further exploration of larger cohorts. Finally, this study lacks statistical significance. A large cohort study of noncardiac surgery reported an in-hospital mortality rate of 4% [35], and we considered a 2% difference clinically significant. In other words, setting the norepinephrine group at 4% and the dopamine group at 6%, a sample size of 1,863 per group was required for 80% power to establish significance. The 1,230-pair one-sided groups in this study corresponded to a power of 62%.
In conclusion, we compared the effects of norepinephrine and dopamine on clinical outcomes in adult patients after noncardiac surgery. Our findings suggest that the advantage of norepinephrine in noncardiac surgery is not as well established as that in the setting of sepsis. Although the results presented in this propensity score analysis provided unique insights into the choice of norepinephrine versus dopamine for blood pressure optimization in noncardiac surgery, further prospective studies are necessary to verify these findings.