Effective concentration of remifentanil for successful i-gel insertion during remimazolam induction
Article information

Abstract
Background
Remifentanil can be used as adjuvants during remimazolam induction without neuromuscular blockade. We evaluated the 95% effective concentration (EC) of remifentanil effect-site concentration (Ce) for the successful insertion of an i-gel using the biased-coin up-and-down method in adult patients during remimazolam induction.
Methods
Forty 19–65 year-old patients scheduled to undergo surgery using i-gel were enrolled. Anesthesia was induced using remimazolam infusion (12 mg/kg/h). Simultaneously, remifentanil was infused at a predetermined Ce. After 5 min of anesthesia induction, the i-gel was inserted. The 95% EC (EC95) of remifentanil in each patient was determined using a biased-coin up-and-down method based on a successful insertion in a preceding patient. The step size of remifentanil Ce was 0.4 ng/ml. If the insertion failed, remifentanil Ce was increased in the next patient. Following successful insertions, the corresponding concentration decreased in subsequent patients with a probability of 1/19 or was maintained with a probability of 18/19. The time from remimazolam infusion initiation to a bispectral index (BIS) < 60 (time to BIS60) and hemodynamic variables were measured and recorded.
Results
The EC95 (95% CI) of Ce was 2.07 (1.94, 2.87) ng/ml. The overall time to BIS60 was 154.0 ± 39.9 s. No patient experienced significant hypotension or bradycardia during remimazolam induction.
Conclusions
The EC95 of remifentanil Ce was 2.07 (1.94, 2.87) ng/ml for successful i-gel insertion during remimazolam induction at 12 mg/kg/h without hemodynamic instability in adult patients. Future studies should measure remifentanil Ce in elderly patients or using remimazolam at various infusion doses.
Introduction
I-gel (Intersurgical Ltd., UK), a type of supraglottic airway, is widely used to maintain the airway during outpatient anesthesia or emergency situations. I-gel is easier to insert and requires less tissue compression than other supraglottic airways with inflatable cuffs [1,2].
Propofol and midazolam are commonly used as intravenous anesthetic agents. However, propofol is associated with hemodynamic instability during anesthesia induction or infusion [3], and midazolam is associated with delayed onset of drug action and delayed recovery [4]. Remimazolam is a recently introduced ultra-short-acting benzodiazepine with a fast onset of action, is degraded by esterase, and has a stable context-sensitive time of 6–7 min even at various infusion times [5,6]. A recent randomized study showed that remimazolam induction (6 and 12 mg/kg/h) was not inferior to propofol induction (2 and 2.5 mg/kg) in terms of efficacy as a general anesthetic sedative [7].
When the operation does not require considerable muscle relaxation during general anesthesia, or when the operation time is short, the surgery can be performed with an airway secured by inserting a supraglottic airway without neuromuscular blockade to ensure a rapid patient recovery. A previous study reported that the use of neuromuscular blocking agents may affect the recovery of patients and delay respiratory function recovery [8]. However, to obtain sufficient anesthetic depth to decrease airway reactivity without neuromuscular blockade, the concentration of sedatives should be increased to a level that may lead to hypotension and bradycardia. To avoid such complications, opioids can be concomitantly used as adjuvants during anesthesia induction [9].
Depending on the type of sedative used, the effective concentration (EC) of effect-site concentration (Ce) for successful insertion during supraglottic airway insertion may vary. However, to date, no study has investigated the EC of remifentanil Ce for successful supraglottic airway insertion during remimazolam induction. Thus, we evaluated the 95% EC (EC95) of remifentanil Ce for the successful insertion of the i-gel without neuromuscular blocking agents using the biased-coin up-and-down method and investigated the hemodynamic changes in adult patients during the induction of 12 mg/kg/h of remimazolam.
Materials and Methods
This study was approved by the Institutional Research Ethics Committee (GDIRB2021-432), registered at https://cris.nih.go.kr (KCT0006968), and was conducted in accordance with the Helsinki Declarartion-2013 and following the receipt of informed consent from each patient after explaining the anesthetic procedure preoperatively. The inclusion criteria included age between 19 and 65 years, American Society of Anesthesiologists (ASA) physical status 1 and 2, and scheduled surgery using i-gel as a supraglottic airway under general anesthesia. Exclusion criteria included patients who had allergies to the drugs used during this study, patients at high risk of aspiration, those expected to experience difficulty in intubation (limited mouth opening, cervical spine extension restriction, or Mallampati class 4), and morbidly obese patients (body mass index > 35 kg/m2).
After the patient arrived in the operating room without premedication, an electrocardiogram, non-invasive blood pressure, and pulse oximeter were installed. A bispectral index (BIS) monitoring device (Covidien LLC, USA) was used to continuously measure the BIS and was attached to the frontal portion of the head. The patients were pre-oxygenated with 100% oxygen for 1 min, followed by an intravenous infusion of remimazolam (12 mg/kg/h). Simultaneously, remifentanil was infused at a predetermined EC using a commercially available target controlled infusion machine (Orchestra®, Fresenius Vial, France). After loss of consciousness (LOC), remimazolam was maintained at 1 mg/kg/h. When consciousness and spontaneous breathing were lost, mask ventilation was provided with 100% oxygen. When the BIS was confirmed to be below 60 after 5 min of anesthesia induction, an i-gel was inserted. Following the manufacturer’s instructions, the anesthesiologist inserted the i-gel in the sniffing position by gently pushing it along the hard palate until resistance was felt. Successful i-gel insertion was defined as proper movement of the chest and a continual end-tidal CO2 tension wave (without air leakage) at a peak airway pressure of < 20 cmH2O. We did not apply positive end-expiratory pressure ventilation in a ventilator setting.
According to the biased-coin up-and-down method, the Ce of remifentanil in each patient was determined based on the successful insertion of the previous patient [10,11]. Assuming that the EC95 is determined (Г = 0.95), the probability Β = 1 – Г / Г = 1 – 0.95 / 0.95 = 1 / 19 is defined. The initial predetermined Ce of remifentanil was 1.5 ng/ml for the first patient because the starting dose should be the minimum dose expected to result in a positive response, that is, close to the expected EC50 [12]. The step size was set as an increment or decrement of 0.4 ng/ml, since the interval between the testing levels should be approximately equal to the standard deviation (SD) [12]. In a previous study, the estimated EC50 (SD) of remifentanil Ce for i-gel insertion during propofol induction using the Dixon’s up-and-down method was 1.58 (0.41) ng/ml [9]. If insertion failed, the Ce of remifentanil was increased in the next patient. However, if the insertion was successful, the Ce of remifentanil was either maintained with a probability of 18/19 or decreased with a probability of 1/19 in the next patient.
The depth of anesthesia was adjusted from a BIS value of 40 to 60, and the time from the start of remimazolam infusion to a BIS < 60 (time to BIS60) was recorded. Hemodynamic variables were measured and recorded before (baseline) and 1 min after anesthesia induction and 1 and 5 min after i-gel insertion. Hypotension was defined as a systolic blood pressure decrease below 80 mmHg or a decrease of > 20% from baseline and was treated with ephedrine (5 mg). Bradycardia was defined as a heart rate < 45 beats/min or a decrease of > 20% from baseline and was treated with atropine (0.5 mg).
The simulation for sample size calculation demonstrated that 20–40 patients were required to obtain the target EC95 with a biased-coin up-and-down design [13]. Moreover, the non-independence and unknown distribution tendency of the up-and-down data require theoretically conservative sample counting to calculate the required number of samples. Previous biased-coin up-and-down studies also demonstrated that a stable target dose can be obtained in 40 patients [14,15]. Therefore, only 40 patients were included in this study.
Statistical analyses were performed using IBM SPSS Statistics software (version 23.0; IBM Inc®, USA) and R code for Windows version 3.2.2 (R Foundation for Statistical Computing®, Austria). Data are presented as the mean ± SD, median (Q1, Q3), or number of patients. The normality of the data distribution was tested using the Kolmogorov–Smirnov test. Continuous data were compared using an independent t-test or repeated measures analysis of variance, as appropriate. The 90% EC (EC90) and EC95 for remifentanil Ce and their CI were estimated using an isotonic regression method with a bootstrapping approach [13,16]. The adjusted response probability was calculated using the pooled-adjacent-violator algorithm (PAVA) [8]. Statistical significance was set at P < 0.05.
Results
Forty patients were enrolled in this study, all of whom completed the trial. Table 1 lists the patient characteristics, and Fig. 1 shows the allocation sequence of Ce according to the biased-coin up-and-down method. Eleven patients were allocated remifentanil at a Ce of 1.5 ng/ml, and the remaining patients were allocated remifentanil at a Ce of ≥ 1.9 ng/ml (1.9 ng/ml, n = 24; 2.3 ng/ml, n = 5). Fig. 2 shows the adjusted success rate from the PAVA. The EC90 (95% CI) of remifentanil and EC95 (95% CI) were 1.86 (1.65, 2.45) and 2.07 (1.94, 2.87) ng/ml, respectively.

Patient Characteristics

The biased-coin up-and-down sequences of remifentanil Ce. Success of i-gel insertion is represented by a filled circle, and failure of i-gel insertion is represented by an open diamond. Ce: effect-site concentration.
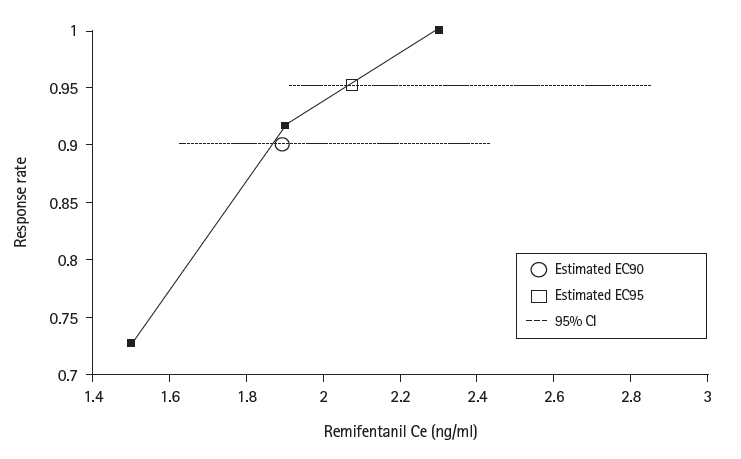
PAVA response rate. The EC90 and EC95 (95% CI) were 1.86 (1.65, 2.45) and 2.07 (1.94, 2.87) ng/ml, respectively. PAVA: pooled-adjacent-violator algorithm, EC: effective concentration.
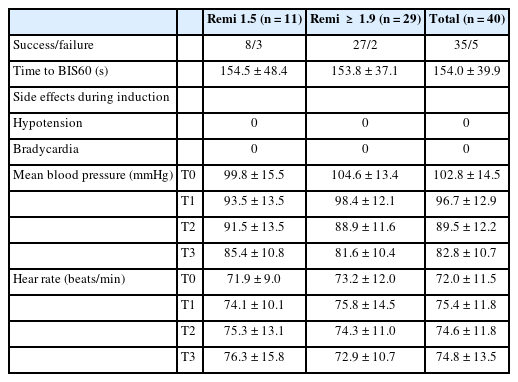
Table 2 lists the induction profiles and hemodynamic changes during remimazolam induction at 12 mg/kg/h. The induction profiles and hemodynamic changes were compared between the patients who were administered 1.5 ng/ml of remifentanil Ce and those who were administered higher than 1.9 ng/ml of remifentanil Ce (1.9 and 2.3), because 1.9 ng/ml of remifentanil Ce was closest to the EC95 value of 2.07 ng/ml in this study (Table 2). The overall time to BIS60 was 154.0 ± 39.9 s, and there were no statistical differences between patients receiving remifentanil Ce of 1.5 and ≥ 1.9 ng/ml. During remimazolam induction, no patients experienced significant hypotension or bradycardia. The changes in the mean blood pressure and heart rate during induction were not significantly different between patients receiving remifentanil Ce of 1.5 and ≥ 1.9 ng/ml (P = 0.09 and 0.43, respectively).
Comparison of Induction Profiles during Remimazolam Induction between Remifentanil Ces
Discussion
This study showed that the EC95 of remifentanil Ce was 2.07 (1.94, 2.87) ng/ml for successful i-gel insertion without neuromuscular blocking agents during the induction of remimazolam at a dose of 12 mg/kg/h in adult patients. Moreover, remimazolam induction had a mean time to BIS60 of 154 s and provided hemodynamic stability during i-gel insertion.
Previous studies have reported various adjuvant drugs, including lidocaine, midazolam, and remifentanil, which enable supraglottic airway insertion with propofol as the induction agent [17]. However, no study has reported an EC of remifentanil that enables supraglottic airway insertion using the newly developed drug remimazolam as an induction agent. Remimazolam is rapidly metabolized by carboxylesterases in the liver and its metabolites have no pharmacological activity [18]. Furthermore, because the effect of remimazolam can be rapidly reversed by flumazenil, it may be safer to use than the inhalation agent or propofol used in the administration of conventional anesthesia [19].
A recent randomized study demonstrated that remimazolam was not inferior to propofol in its efficacy as a sedative for anesthesia induction [7]. In this study, anesthesia was induced by injecting remimazolam at a rate of 12 mg/kg/h. Several studies have been conducted to evaluate the EC50 and EC95 of Ce, which enables i-gel or laryngeal mask airway insertion during propofol induction without neuromuscular blockade. Jeon et al. [20] reported that, by applying Dixon’s up-and-down method, the EC95 of remifentanil for successful i-gel insertion was 2.44 and 0.75 ng/ml during 4.0 and 6 μg/ml of propofol induction, respectively, in patients who are expected to have difficult airways. Another study, which also applied Dixon’s method identified an EC95 2.38 ng/ml for remifentanil to enable i-gel insertion without the use of muscle relaxants during a propofol induction of 4.0 μg/ml Ce in female patients [9]. In this study, the EC95 (95% CI) of remifentanil for i-gel insertion was 2.07 (1.94, 2.87) ng/ml during an anesthetic induction of remimazolam at a dose of 12 mg/kg/h without neuromuscular blockade. This result is similar to the EC95 of remifentanil measured during induction at a 4.0 μg/ml propofol Ce reported in a previous study but showed a lower level.
The Dixon up-and-down method used in the studies described above was designed to determine EC50 by simplifying a biased-coin design, which can also be used for approximating EC95 using logistic or probit regression [10]. However, if the quartile is higher, the extrapolated EC95 obtained using the Dixon up-and-down method may impose a significant bias [10]. In contrast, when a biased-coin design is adapted, the EC can be estimated at any quartile [10]. In practice, the EC50 value of a drug to determine its dose is limited. This is because the effectiveness should be achieved in 90–95% of patients, rather than only 50% [21]. Furthermore, when measuring the EC95 dose of a drug with a biased-coin design, the distribution of most administered doses tends to peak around the mean and adverse effects that may occur with EC95 can be confirmed [13]. Therefore, in this study, a biased-coin design was used to approximate the EC95 of remifentanil for i-gel insertion, without the use of muscle relaxants during induction with remimazolam.
In this study, stable hemodynamic conditions were maintained during induction and after i-gel insertion. No patient developed hypotension or bradycardia. The half-life of propofol is short and recovery is rapid; however, it is associated with the potential for respiratory depression and hypotension [22]. According to previous studies, the incidence of hypotension was lower with remimazolam than with propofol [7,22–24]. In patients with gastric cancer undergoing robotic gastrectomy, a significantly reduced amount of vasopressor was observed in the group anesthetized with remimazolam than in the group anesthetized with sevoflurane, and a higher mean blood pressure was maintained intraoperatively [25]. Another study on patients undergoing colonoscopy reported a significantly lower incidence of hypotension in the remimazolam group than in the midazolam group [26]. Chen et al. [27] reported that the incidence of respiratory depression was significantly lower in the remimazolam group than in the propofol group [27]. Therefore, when remimazolam is used during induction, i-gel insertion is expected to be possible while maintaining stable hemodynamics compared to conventional drugs.
This study had several limitations. First, because a fixed infusion rate of remimazolam was used, the effects of other remimazolam infusion rates and dosages on the Ce of remifentanil could not be measured. Future studies should measure Ce using remimazolam at various infusion rates and doses. Second, this study only included relatively healthy patients with ASA physical status 1 or 2 aged 19–65 years, and patients with various diseases and older patients might show different hemodynamic responses to the drug. Therefore, the results may not be generalizable to all adults. However, our findings may also provide predictive indicators for drug demand in other patients. Third, although the time to LOC is also an important characteristic of sedatives, we missed checking the time to LOC during remimazolam induction of 12 mg/kg/h.
In conclusion, the EC95 of remifentanil Ce for successful i-gel insertion without neuromuscular blocking agents was 2.07 (1.94, 2.87) ng/ml during remimazolam induction at a dose of 12 mg/kg/h in adult patients. Moreover, remimazolam induction could provide hemodynamic stability during i-gel insertion. Future studies should measure remifentanil Ce in elderly patients or using remimazolam at various infusion doses.
Notes
Funding
None.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
Jung Ju Choi (Data curation; Formal analysis; Investigation; Project administration; Resources; Visualization; Writing – original draft)
Wol Seon Jung (Resources; Writing – review & editing)
Young Jin Chang (Software; Writing – review & editing)
Seungbeom Yoo (Resources; Writing – review & editing)
Hyun Jeong Kwak (Conceptualization; Data curation; Investigation; Methodology; Software; Supervision; Validation; Writing – original draft)