Introduction
Postoperative nausea and vomiting (PONV) is an important consideration in postoperative management as it is associated with significant patient distress. Many studies designed to identify potential risk factors for PONV have been conducted [1–3]. The type of general anesthetic agent used is one potential risk factor that can significantly influence the likelihood of PONV [1–3]. Specifically, total intravenous anesthesia (TIVA) has a lower incidence of PONV than inhalational anesthesia [1–3]. Propofol is typically used as an intravenous general anesthetic agent because its duration of action is shorter than that of conventional benzodiazepines, which are associated with delayed awakening and resedation [4].
Remimazolam, an ultrashort-acting benzodiazepine, has recently become available for general anesthesia and procedural sedation. Compared with propofol, remimazolam is associated with a lower incidence of hypotension [5] regardless of the patient’s American Society of Anesthesiologist Physical Status (ASA-PS) classification or age [6]. However, the incidence of PONV during TIVA with remimazolam has not been well investigated in clinical settings. A higher incidence of nausea or vomiting has been reported with remimazolam anesthesia than with propofol anesthesia in clinical trials [6]. We hypothesized that the incidence of PONV would be higher after TIVA with remimazolam than with propofol. In this propensity score-matched, retrospective, observational study, we compared the rates of PONV between remimazolam and propofol.
Materials and Methods
Study design, setting, and participants
This propensity score-matched, retrospective, observational, single-center cohort study was approved by the Clinical Research Ethics Committee of the Hamamatsu University School of Medicine (IRB no. 21–169). All the procedures were conducted in accordance with the Helsinki Declaration-2013. The requirement for written informed consent was waived due to the retrospective nature of the study and anonymity of the data. However, information about the study was posted on the hospital’s noticeboard and website to give patients the opportunity to opt-out of the study. The study was registered in the Japan Registry of Clinical Trials (jRCT1041210079). All patients who received general anesthesia at Hamamatsu University Hospital between August 2020 and July 2021 were eligible for inclusion. The exclusion criteria were as follows: aged < 20 years, surgery with sedation rather than general anesthesia, postoperative mechanical ventilation, discontinuation of surgery after induction of anesthesia, stupor or coma lasting more than 24 h after anesthesia, reoperation within 24 h after anesthesia, insufficient data, combined use of propofol and remimazolam, and use of inhalational anesthetics. The remimazolam group included patients who received only remimazolam and no other anesthetic agents (e.g., midazolam, thiopental, propofol, or inhalational anesthetics) during the entire anesthesia period from induction to recovery. Likewise, only patients who received no anesthetic other than propofol during the anesthesia period were included in the propofol group.
Outcomes and measurements
The primary outcome of the study was the incidence of PONV, which was defined as nausea and/or vomiting within 24 h of general anesthesia. The secondary outcome was the relationship between potential risk factors and the incidence of PONV. All data were obtained from the surgical department system linked to the anesthesia records (ERGATM, Philips Japan, Japan) and hospital information system (MegaOakTM, NEC, Japan). The study was conducted in a facility that does not have a day surgery unit. Therefore, all patients undergoing surgery requiring general anesthesia are admitted for at least one night of postoperative care and, in most cases, are discharged on the second postoperative day. All patients at this facility are also required to undergo a postoperative medical examination by an anesthesiologist before discharge. This check is usually scheduled for the second postoperative day. The anesthesiologist briefly examines the patient for any anesthesia-related complications, including PONV, and records the timing and severity in the patient’s electronic medical record. Patients who are unable to be examined by an anesthesiologist prior to discharge are interviewed by telephone. Data from the electronic medical records of all the study participants were reviewed retrospectively to confirm whether PONV occurred within the first 24 h. Patients who did not undergo a postoperative evaluation by an anesthesiologist were excluded from the study.
Sample size
To calculate the sample size, the incidence of PONV after TIVA with propofol was set at 15% in accordance with the findings of Kampmeier et al. [7]. Because the incidence of PONV after TIVA with remimazolam has not been reported previously, we used an expected incidence of 25%, which has been confirmed in clinical trials conducted in Japan (phase II/III trial, ONO-2745-05; phase III trial, ONO-2745-06) (Supplementary Materials 1 and 2). Thus, we estimated that at least 249 cases per group would be required to achieve a study power of 80% to detect the primary outcome for the remimazolam group versus the propofol group using a two-sided χ2 test at a significance level of P < 0.05. At our institution, inhaled anesthesia is currently being used approximately twice as often as TIVA, though the frequency of remimazolam use is comparable to that of propofol. Additionally, we estimated that approximately one-third of the patients would be excluded during propensity score matching; therefore, we chose a study period of 1 year, which included approximately 5,000 patients.
Bias and confounding
Individual propensity scores were calculated using logistic regression modeling based on the following covariates, which were considered to be directly or potentially related to the choice of remimazolam or propofol anesthesia: demographics (age, female sex, obesity [body mass index ≥ 25 kg/m2]), type of surgery (abdominal, laparoscopic, gynecologic, orthopedic), anesthesia-related factors (ASA-PS, duration of surgery, use of nitrous oxide, intraoperative use of fentanyl and remifentanil, postoperative use of fentanyl), and other factors (smoking history and whether surgery was elective). Patients were matched 1 : 1 with their nearest neighbors according to the closest propensity score of each subject. A caliper size of 0.2 was used to avoid poor matching.
Statistical analysis
Categorical data are presented as absolute numbers (percentages) and continuous data are presented as the mean ± SD. Differences in the characteristics of patients with and without PONV were examined using the Student’s t-test or Fisher’s exact test, as appropriate.
To assess the relationship between potential risk factors and the incidence of PONV (secondary outcome), the following variables were evaluated: age [3,8], sex [2,3,8], obesity [2], type of surgery (abdominal [2], laparoscopic [2,3], gynecologic [2,3], orthopedic [2]), duration of surgery [2,3,8], ASA-PS 1–2 [2], intraoperative administration of fentanyl and remifentanil [2,8,9], postoperative administration of fentanyl [2,3,8], smoking history [2,3,8], urgency of surgery [10], use of dexamethasone [1], use of droperidol [1], and remimazolam anesthesia. We could not investigate whether patients had a previous history of PONV or motion sickness because it was not documented in the electronic medical records. The association between each factor and PONV was examined using logistic univariate analysis. Odds ratios (ORs), 95% CIs, and Wald’s P values were calculated. A logistic regression analysis was then performed using the stepwise selection method with these covariates as explanatory variables and PONV as the outcome variable. The following six covariates were identified as explanatory variables for PONV: female sex, laparoscopic surgery, intraoperative fentanyl use, smoking, droperidol use, and remimazolam anesthesia. Adjusted ORs (aORs), 95% CIs, and Wald’s P values were calculated.
All P values were two-sided, and a P value < 0.05 was considered statistically significant. All statistical analyses were performed using JMP for Windows (version 14.2.0, SAS Institute Inc., USA).
Results
From August 2020 to July 2021, 4,933 patients underwent general anesthesia according to the surgical record system of the Hamamatsu University Hospital. After 3,694 were excluded based on the aforementioned eligibility criteria, the study population consisted of 1,239 patients (585 in the remimazolam group and 654 in the propofol group). Nearest-neighbor matching was performed to match each patient with a suitable counterpart, after which 666 patients were matched into 333 pairs (Fig. 1). Patient characteristics and PONV rates before and after matching are presented in Tables 1 and 2, respectively. The absolute standardized difference after matching for all the variables ranged from 0.000 to 0.090, with an absolute standardized difference < 0.1 indicating that the allocation of both groups by propensity score matching was performed appropriately.
The incidence of PONV in the remimazolam anesthesia group was significantly higher than that in the propofol anesthesia group both before matching (27% [158/585] vs. 22% [142/654], P = 0.034) and after matching (35% [116/333] vs. 21% [70/333], P < 0.001). The incidence of PONV in the remimazolam group before matching was 27% [145/544] with flumazenil and 32% [13/41] without flumazenil; however, the difference was not statistically significant (Table 3).
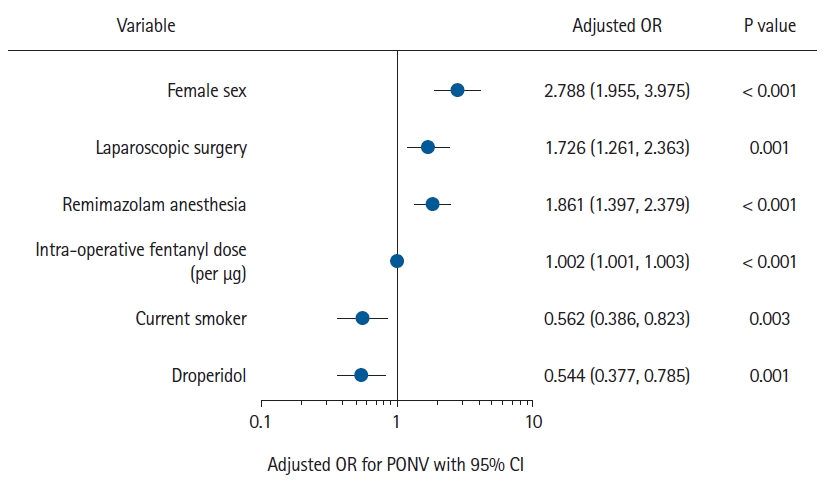
Table 4 shows the results of the univariate and logistic regression analyses for the incidence of PONV using the stepwise selection method. Female sex, laparoscopic surgery, intraoperative fentanyl use, smoking, droperidol use, and remimazolam anesthesia were significantly associated with the development of PONV (Table 4). The strengths of each risk factor for PONV are shown in Fig. 2.
Discussion
In this retrospective observational cohort study, the risk of PONV associated with remimazolam and propofol TIVA was evaluated using the propensity score matching method. Our results showed that the incidence of PONV was significantly higher in the remimazolam group than in the propofol group (35% vs. 21%). This suggests that remimazolam anesthesia is associated with a higher risk of PONV than propofol anesthesia. To the best of our knowledge, this is the first study with sufficient power to compare the incidence of PONV after anesthesia with remimazolam vs. propofol.
We performed a propensity score-matched analysis to compare remimazolam and propofol in order to eliminate the potential effects of covariates on the risk of PONV. Using this method, we observed a significant difference in the rate of PONV between remimazolam and propofol. Since the TIVA protocol was otherwise the same, we speculate that this difference can be explained by the antiemetic effects of propofol and/or benzodiazepines. As Hvarfner et al. [11] have previously argued, propofol can exert an antiemetic effect when administered at a concentration lower than that which results in sedation. After awakening from general anesthesia, the concentration of propofol that remains in the patient’s body is less than the level required for sedation and thus could have an antiemetic effect. Hvarfner et al. [11] also reported the antiemetic effects of midazolam, and a meta-analysis found that midazolam reduced the incidence of PONV [12]. After remimazolam is administered, the sedation effect dissipates quickly because remimazolam is rapidly degraded by carboxylesterases in the liver and the pharmacological activity of its metabolite CNS-7054 becomes negligible [13]. There are two possible explanations for the reduced antiemetic effect associated with benzodiazepines in this study. One is that remimazolam degrades more rapidly than conventional benzodiazepines, and the other is that administering flumazenil after remimazolam eliminates the antiemetic effect by competitive antagonism. Either or both of these factors may explain why the incidence of PONV was higher with remimazolam than with propofol.
Several studies have confirmed the risk of PONV following anesthesia, and guidelines have been developed for its prevention [1,14]. While TIVA is one such method, the risk of PONV associated with remimazolam specifically has not been well-studied. Therefore, risk factors for PONV other than remimazolam anesthesia were also investigated in the present study. We found that female sex and laparoscopic surgery were associated with a significantly higher incidence of PONV. This is consistent with the PONV management guidelines [1], a review article [2], and a systematic review [3]. The present study also confirmed that a history of smoking and droperidol use reduced the risk of PONV [1,14]. Furthermore, our study showed that an increase in the intraoperative fentanyl dose correlated with an increased incidence of PONV, which is consistent with a report by Mauermann et al. [9]. These results are consistent with previous findings [1–3,8,9,14] and suggest that the current study was conducted appropriately. Dexamethasone is an important prophylactic agent for PONV [1,14,15]. However, the OR for dexamethasone was not significant in either the univariate or logistic regression analysis in our study. It is possible that this result reflects a lack of statistical power, considering that dexamethasone was administered to only 26 of the 1,239 patients included in this study. A previous meta-analysis found that to prevent PONV within 24 h, the number needed to treat (NNT) for dexamethasone is 3.7–3.8 [15]. However, cases of inhalation anesthesia were included in this meta-analysis, and thus, its findings cannot be compared directly with those of the present study. Therefore, we compared our results with those of a randomized controlled trial investigating the ability of dexamethasone to prevent PONV after TIVA with propofol that included 40 patients each in the dexamethasone and placebo groups [16]. In that study, the NNT for the prevention of PONV with dexamethasone was 5. Extrapolating the results of that trial to our present study and performing a power analysis with an NNT of 5 and significance level of 0.05, with 26 cases in the dexamethasone group, 1,213 cases in the control group, and a 24% rate of PONV in the group that did not receive dexamethasone, the power was calculated to be 0.649. Therefore, it seems reasonable to attribute the failure of our study to detect dexamethasone’s capacity to prevent PONV to an insufficient number of cases.
Assuming that remimazolam anesthesia increases the incidence of PONV to a similar extent as female sex and laparoscopic surgery, as demonstrated in this study, precautions should be taken to prevent PONV associated with remimazolam anesthesia or to avoid its use. Whether remimazolam should be recommended as an alternative to propofol in TIVA to prevent PONV remains unclear. Mao et al. [17] found no statistically significant difference in the incidence of PONV after urological surgery according to whether remimazolam or propofol was used (10.9% vs. 4.7%). However, they concluded that their sample size was inadequate and further studies are needed. Studies comparing the rate of PONV after remimazolam anesthesia with that after propofol anesthesia are currently underway (UMIN000039367 [18], UMIN000040944 [19], UMIN000044442 [20], UMIN000046237 [21], NCT05439057 [22]), and their results are anticipated. Comparisons of the incidence of PONV between remimazolam and inhaled anesthetic agents have also been reported. Hari et al. [23] found that the incidence of early PONV was lower after the administration of remimazolam than after the administration of desflurane in patients undergoing laparoscopic gynecologic surgery. Song et al. [24] also demonstrated that the incidence of early PONV was lower with remimazolam than with desflurane in patients undergoing laparoscopic cholecystectomy or robot-assisted gynecological surgery. These findings, although limited, indicate that PONV is less likely to occur with remimazolam than with inhaled anesthetic agents. Overall, we could assume that the risk of PONV with remimazolam anesthesia is higher than that with propofol anesthesia and lower than that with inhaled anesthetic agents.
Several factors besides those associated with anesthesia affect the incidence of PONV. For example, gastrointestinal surgery has been linked to a higher incidence of nausea and vomiting because of decreased intestinal peristalsis in response to surgical invasion of the intestinal tract [25]. In the present study, after adjusting for the rates of abdominal surgery and laparoscopic surgery, we evaluated the effects of different anesthetic agents on the incidence of PONV. However, we did not adjust for other surgical procedures, such as strabismus surgery [26] and otolaryngologic surgery [8], which are associated with a higher incidence of PONV. In the future, the effects of remimazolam on PONV should be investigated for each type of surgery.
This study has several limitations. First, the major risk factors for developing PONV, including motion sickness and a previous history of PONV [2,3], were not investigated. Therefore, the risk of developing PONV may not have been accurately adjusted for, even after propensity score matching. Second, our evaluation of PONV was based only on a binary assessment of its presence or absence; differences in severity and timing were thus not considered. Third, when an antiemetic agent was not administered, each patient’s subjective response in the postoperative interview was used to determine whether postoperative nausea was present. Therefore, postoperative nausea may not have been communicated to the evaluator or may not have been recalled by the patient. Finally, because this study was based on a retrospective review of electronic records, it was impossible to identify and remove any errors in the data.
Bivariate analysis with adjustment using the propensity score matching method revealed that patients who received total intravenous general anesthesia with remimazolam had a higher incidence of PONV than those who received propofol. To the best of our knowledge, this is the first study to demonstrate a higher incidence of PONV after remimazolam anesthesia than after propofol anesthesia. However, because of the retrospective design of this study, caution is required when generalizing the results. Larger prospective randomized controlled trials are needed to confirm these findings.