Introduction
Within the body’s circulatory system, the desynchronization between macrocirculation and microcirculation, such that the restoration of systemic circulation does not ensure the restoration of microcirculatory perfusion and oxygenation of the tissues, is called ‘microcirculatory shock’ [1,2]. Numerous studies have shown that microcirculatory shock is significantly associated with poor clinical outcomes in patients with sepsis [3–5]. However, most studies related to microcirculation in cardiac surgeries are insufficient to conclusively establish the associations between microcirculatory dysfunction and clinical outcomes. Notably, some studies have shown a correlation between microcirculatory dysfunction and major adverse events (MAE) such as stroke [6], myocardial infarction (MI) [7], heart failure [8], acute kidney injury (AKI) [9], gastrointestinal (GI) bleeding [10], and acute respiratory distress syndrome (ARDS) [11].
Ample studies have been conducted on microcirculation in patients undergoing cardiac surgeries and sepsis patients, because they are at an increased risk of microcirculatory shock [12,13]. The patients undergoing cardiac surgeries are typically older adults with comorbidities. Cardiac surgery causes systemic inflammation and endothelial dysfunction induced by the production of free radicals and inflammatory mediators, complement activation, and ischemia/reperfusion injuries [4,14]. Excessive transfusions, fluids, and vasopressors can negatively affect microcirculation [15,16]. Cardiopulmonary bypass (CPB)-induced microcirculatory perfusion disturbances have been demonstrated in several studies [13,17]. The observed microcirculatory perfusion disturbance was largely absent in the patients undergoing off-pump surgeries [17]. Another study showed that microcirculatory alterations decreased with time but persisted for > 24 h post on-pump cardiac surgeries [13]. Interestingly, the extent of the microvascular changes seems related to tissue ischemia and correlated with the peak lactate levels post-surgery. This data suggests that impaired microvascular perfusion contributes to organ dysfunction following CPB. The preservation of microcirculatory perfusion may thus improve clinical outcomes.
Therefore, several studies have investigated whether microcirculatory shock in cardiac surgeries correlates with the postoperative outcomes using a vascular occlusion test (VOT) with near-infrared spectroscopy (NIRS) [18–21]. Some studies have found that the recovery slope of VOT (representing the microvascular reactivity) in the intensive care unit (ICU) post-surgery was associated with postoperative outcomes [19,20]. However, predicting the postoperative outcomes as early as possible is beneficial for adopting intraoperative preventive strategies.
We hypothesized that if the microvascular reactivity is preserved during CPB, tissue hypoxemia can be minimized. In contrast, in the patients with disturbed microvascular reactivity during CPB, tissue hypoxemia develops, which may lead to poor clinical outcomes. The primary aim of this study was to assess whether the microvascular reactivity during CPB can predict MAE post-cardiac surgery. Additionally, the association of these microcirculatory parameters with other postoperative clinical outcomes, including the Sequential Organ Failure Assessment (SOFA) score, Acute Physiologic and Chronic Health Evaluation (APACHE) II score, duration of ventilator care, length of ICU stay, and length of hospital stay, was investigated. Finally, the additional risk factors for MAE after cardiac surgery were investigated.
Materials and Methods
Patients
This study was approved by the Institutional Review Board (Pusan National University Hospital, Busan, Republic of Korea, No. 1702-003-051, date of approval 10/02/2017), and written informed consent was obtained from all participants on the day before surgery. This study was conducted in accordance with the ethical principles of the Helsinki Declaration-2013 and followed good clinical practice guidelines. This prospective, observational, single-center study was conducted between February 2017 and May 2019 at a tertiary university hospital. The study adhered to the applicable STROBE statement. Adult patients aged > 18 years who were scheduled for elective on-pump cardiac surgeries were included. The exclusion criteria were pregnancy, the inability to tolerate VOT (e.g., patients with arm deformities, arteriovenous shunts, and burns), or refusal to participate in the study.
Anesthesia
The standard monitoring for cardiac surgery was performed in the operating room, which consisted of the following: electrocardiography, arterial blood pressure, pulse oximetry, rectal temperature, bispectral index (BIS), cerebral oximetry, pulmonary artery catheterization (PAC), and transesophageal echocardiography. General anesthesia was induced using 1.0–1.5 mg/kg propofol and a continuous infusion of 0.1 μg/kg/min remifentanil. After the injection of 0.8 mg/kg rocuronium, tracheal intubation was performed, and mechanical ventilation was commenced with an inspired oxygen fraction (FiO2) of 0.5, tidal volume of 6–8 ml/kg, and respiratory rate adjusted to maintain an end-tidal CO2 of 30–35 mmHg. The general anesthesia was maintained using sevoflurane and remifentanil to sustain a BIS ranging between 40 and 60 during the surgical procedure, including CPB. The hemodynamic parameters were maintained within 20% of the baseline values. A packed red blood cell (pRBC) transfusion was administered to maintain a hemoglobin level of 8–10 g/dl. Treatments using fresh frozen plasma, cryoprecipitate, and platelets were considered in case of insufficient surgical coagulation following the normalization of activated clotting time (ACT). The decision to administer vasopressors and inotropes was made by the attending physicians based on the hemodynamic status evaluation.
A Sorin Stockert C5 or S5 heart‐lung machine with a centrifugal blood pump and heater‐cooler device (Sorin Stockert Instrumente GMBH, Germany) was used for bypass with a phosphorylcholine-coated extracorporeal circuit (Phisio, LivaNova, Italy). The non-pulsatile CPB technique was used with a membrane oxygenator primed with 1,000 ml plasma solution, 250 ml 15% mannitol, 40 ml 8.4% sodium bicarbonate, 100 ml 20% albumin, 20 ml 10% magnesium sulfate, 2 g tranexamic acid, 120,000 units Ulinastatin, 1 g methylprednisolone, 5,000 IU bovine heparin, and 1 g cefazolin. CPB was initiated after heparin administration (300 IU/kg), when the target ACT exceeded 480 s. Myocardial protection was achieved using a 4°C Del Nido solution. The pump flow rate was calculated based on the patient’s body surface area and subsequently maintained to ensure a mean arterial pressure (MAP) of 60–80 mmHg with mild-to-moderate hypothermia (28–35°C). After weaning from CPB, protamine was administered in a 1 : 1 ratio, in addition to 2 g of tranexamic acid to achieve normal ACT.
In the ICU, patients were sedated with dexmedetomidine and remifentanil until the following extubation criteria were met: the patient could obey commands, was stable, and had adequate hemodynamics, insignificant arrhythmia, chest tube drainage < 100 ml/h for two consecutive hours, an arterial partial pressure of carbon dioxide (PaCO2) < 50 mmHg, arterial partial pressure of oxygen (PaO2) ≥ 70 mmHg with FiO2 ≤ 50%, and urine output ≥ 1 ml/kg/h.
VOT
The VOT was performed five times in each patient: before the induction of general anesthesia (baseline, T0), 30 min after the induction of general anesthesia (T1), 30 min after application of CPB (T2), 10 min after protamine injection (T3), and after sternal closure (T4). Before the induction of anesthesia, an NIRS sensor (INVOSTM 5100C Cerebral/Somatic Oximeter; Medtronic, USA) was placed on the thenar eminence and an automated tourniquet (A.T.S® 3000 Automatic Tourniquet System; Zimmer Inc., USA) was placed around the upper arm. The arterial catheter was placed in the contralateral radial artery, and the baseline blood pressure was measured. When the baseline tissue oxygen saturation (StO2) stabilized, the automatic tourniquet was inflated to 50 mmHg over the patient’s baseline systolic blood pressure and maintained for 5 min. After a 5 min ischemic period, the tourniquet deflated rapidly. The StO2 data was recorded continuously during the VOT procedure. The baseline StO2, minimum StO2 during the 5 min tourniquet inflation, and maximum StO2 during tourniquet deflation were obtained. The occlusion and recovery slopes were calculated based on the measured StO2 data. The occlusion slope, related to the oxygen extraction, was defined as the slope of the StO2 descent to the lowest value. The recovery slope, related to the microvascular reactivity, was calculated from the deflation of the tourniquet until the StO2 recovery reached the highest value. As the range of StO2 measurable by the INVOSTM is 15–95%, the occlusion and recovery slope calculations were made using 15% as the lowest value and 95% as the highest value, even when the actual values exceeded this range.
Intraoperative data collection
All the data was recorded at five distinct time points, as described previously. The hemodynamic data was obtained using standard monitoring. The systemic vascular resistance (SVR) was calculated using the measured MAP, central venous pressure (CVP), and cardiac output (CO) using the following equation: SVR = (MAP − CVP) / CO × 80. Arterial blood gas analysis was performed to obtain the PaO2, PaCO2, hemoglobin, and lactate levels. After weaning from CPB at T3 and T4, the vasoactive-inotropic score (VIS) was calculated as follows: dopamine dose (mg/kg/min) + dobutamine dose (mg/kg/min) + 100 × epinephrine dose (mg/kg/min) + 10 × milrinone dose (mg/kg/min) + 10,000 × vasopressin dose (unit/kg/min) + 100 × norepinephrine dose (mg/kg/min) [22]. Post-CPB vasoplegia was defined as MAP < 65 mmHg with a cardiac index > 2.2 L/kg/m2 and SVR < 800 dyne/s/cm5 [23].
Postoperative outcomes
The SOFA and APACHE II scores were assessed in the ICU. Both were calculated within 24 h after ICU admission, and the SOFA score was calculated daily until ICU discharge. Additionally, the duration of ventilator care, ICU stay, and hospital stay were recorded. All postoperative MAE within 30 days post-surgery were recorded. The patients were routinely scheduled to visit the clinic two weeks post-discharge and instructed to visit the emergency center at the occurrence of any MAE. The MAE included death, aggravated heart failure, MI, AKI, stroke or seizure, ARDS, and GI bleeding. Aggravated heart failure was defined as an increase in the functional class or left ventricular ejection fraction of < 35%. MI was defined by elevated cardiac troponin (cTn) values > 10 × 99th percentile upper reference limit (URL) in patients with normal baseline cTn values (< 99th percentile URL), in addition to either: (a) new pathological Q waves or new left bundle branch block, (b) angiography-documented new graft or new native coronary artery occlusion, or (c) imaging evidence of recent loss of viable myocardium or new regional wall motion abnormalities [24]. AKI was defined in accordance with the Kidney Disease Improving Global Outcomes definition, i.e., 0.3 mg/dl increase in serum creatinine over 48 h or 1.5 times higher than the baseline value within 7 days post-surgery [25]. ARDS was defined as the PaO2/FiO2 ≤ 300 mmHg with a positive end-expiratory pressure or continuous positive airway pressure ≥ 5 cmH2O. These pressures were associated with bilateral opacities on chest imaging, not fully explained by effusions and lobar/lung collapse or nodules and not fully explained by cardiac failure or fluid overload [26].
Statistical analysis
The primary outcome of this study was the predictive value of the recovery slope of VOT during CPB. Based on our pilot study consisting of 20 patients before enrollment, three patients had MAE (15%), and the area under the receiver operating characteristic (AUROC) curve was 0.723. A power calculation determined a sample size of 104 patients with two-sided α risk of 5%, β risk of 20%, and positive/negative ratio of 5.5. Considering the dropout rate of 10%, 115 patients were required for the study.
The data is expressed as frequencies (%), median (Q1, Q3), or mean ± SD. All the continuous variables were tested for normality using a Q–Q plot and Kolmogorov–Smirnov test. Continuous variables were compared using independent t-tests or Mann–Whitney U tests. Categorical variables were compared using the chi-squared or Fisher’s exact tests. The intraoperative VOT, hemodynamic, and laboratory data were compared using two-way repeated-measures analysis of variance (ANOVA). For the intra-subject factor analysis, either ANOVA or Friedman analysis was performed. For post hoc tests of inter-subject factors, the Bonferroni correction was used. Appropriate adjustments for Bonferroni correction are stated in the tables with multiple P value comparisons.
The patients were divided according to post-surgery MAE. The VOT variables that were significantly different between the two groups were tested for accuracy of predicting MAE using the ROC curve with a 95% CI. The AUROC was compared using a method previously used by DeLong et al. [27]. The optimal cutoff value was selected to maximize the Youden index. Patients were divided according to the optimal cutoff. The incidence of post-CPB vasoplegia and postoperative outcomes were compared. The association between the occurrences of MAE was analyzed using univariate and multivariate logistic regression analyses. The factors significantly associated with MAE were selected for the univariate analysis (P < 0.05). The Spearman’s correlation coefficients were computed to evaluate collinearity (r > 0.7). If correlation was found between the variables, the ones most relevant from a clinical perspective were chosen. The candidate variables were entered into a forward stepwise multivariate logistic regression model. The model was evaluated using a −2 log-likelihood ratio, Nagelkerke R2, Hosmer–Lemeshow test, and predicted probabilities. Statistical significance was set at P < 0.05. The data analyses were performed using MedCalc® Statistical Software version 19.5.3 (MedCalc Software Ltd., Ostend, Belgium) and SPSS statistics software (IBM SPSS Statistics for Windows, Version 25.0, Armonk, NY, USA).
Results
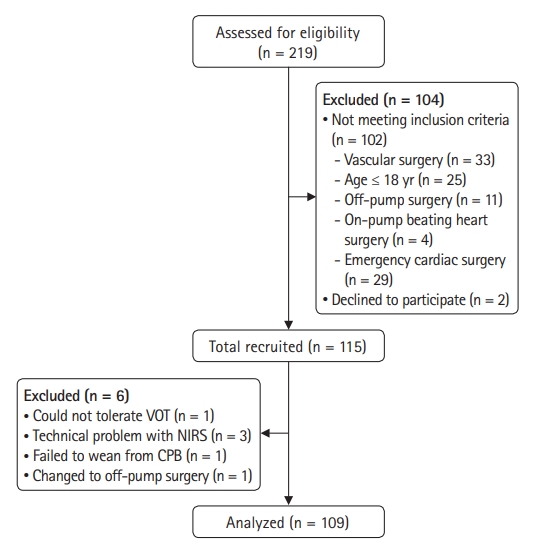
Of the 219 eligible patients, 115 were included in the study. Six patients were excluded for the following reasons: could not tolerate the VOT (n = 1), technical problems with NIRS (n = 3), failed weaning from CPB (n = 1), and changed to off-pump surgery (n = 1) (Fig. 1). The patient demographics and intraoperative characteristics are summarized in Table 1. Of the 109 patients, MAE occurred in 32 (29.4%). The patients who experienced MAE underwent valvular surgery more frequently. Hypertension and chronic kidney disease were more common, and the EuroSCORE II was significantly higher in the patients with MAE. The surgery durations, anesthesia, CPB, and aortic cross-clamping were significantly longer in the patients with MAE. Additional pRBC transfusions were required, and the urine output was lower in patients with MAE. After weaning from CPB, more vasopressors and inotropes were administered. Additionally, post-CPB vasoplegia developed more frequently in the patients with MAE.
The hemodynamic and laboratory data are presented in Supplementary Table 1. Baseline hemoglobin and lactate levels were significantly lower in the patients with MAE. The MAP decreased after CPB application, and the HR, CI, and serum lactate levels increased after weaning from CPB. The SVR decreased significantly after weaning from CPB. The rectal temperature was markedly lower and PaO2 was markedly higher during CPB. Table 2 summarizes the VOT variables at the five specified time points. The MAE were as follows: death (3.7%), aggravated heart failure (4.6%), MI (1.8%), AKI (22.9%), stroke or seizure (4.6%), ARDS (1.8%), and GI bleeding (1.0%). Most MAE developed within 7 days post-cardiac surgery. Nearly 30 days after surgery, one case of aggravated heart failure and two cases of death occurred.
For the primary outcome, the AUROC of the VOT variables for predicting the post-surgery MAE has been presented in Table 3. The AUROC for the recovery slope during CPB was 0.701 (P < 0.001; 95% CI [0.606, 0.785]). If the recovery slope during CPB was ≤ 1.08%/s, MAE were predicted with a sensitivity of 62.5% and specificity of 72.7%. The AUROC of the recovery slope during CPB was not significantly different from other AUROC associated with the other VOT variables.
The patients were divided according to the cutoff value of the recovery slope during CPB, and the incidences of post-CPB vasoplegia and postoperative outcomes were compared (Table 4). The patients with a recovery slope < 1.08%/s during CPB had a higher maximum SOFA score and longer duration of ventilator care. MAE, particularly postoperative AKI, developed more frequently in the patients with lower recovery slopes during CPB.
As shown in Table 5, we identified the risk factors for post-cardiac surgery MAE using logistic regression analysis. The P value of the Hosmer–Lemeshow test of the model was 0.676. The model had −2 log-likelihood of 77.1, Nagelkerke R2 of 0.564, and predicted probabilities of 85.3%. According to the multivariate analysis, the independent risk factors for MAE were hemoglobin at T1 (odds ratio [OR]: 0.604, 95% CI [0.433, 0.842], P = 0.003), CPB duration (OR: 1.022, 95% CI [1.007, 1.038], P = 0.005), intraoperative urine output × 0.1 (OR: 0.988, 95% CI [0.978, 0.998], P = 0.015), VIS at T3 (OR: 1.097, 95% CI [0.978, 0.998], P = 0.012), and recovery slope at T2 (OR: 0.220, 95% CI [0.076, 0.635], P = 0.005).
Discussion
This study found that the microvascular reactivity during CPB could be a predictive factor for the occurrence of postoperative MAE. Patients with recovery slopes ≤ 1.08%/s during CPB had higher maximum SOFA scores in the ICU and longer durations of ventilator care. Additionally, MAE developed more frequently in these patients.
Only one previous study investigated the predictive value of VOT variables during CPB for postoperative outcomes, such as the length of ICU stay and SOFA scores, and reported negative results [18]. However, since they only analyzed 40 patients, the study may have lacked sufficient statistical power. Moreover, VOT was performed using the StO2-targeted method, wherein the cuff was deflated upon reaching 40% of the baseline. We used the 5 min time-targeted VOT method, wherein most patients reached StO2 values of 15%, the lowest possible value measurably by INVOSTM. The difference in the recovery slopes between patients with and without MAE was significant in our study because smaller minimum StO2 values after ischemia result in more defined recovery slopes [28,29].
Other studies have performed VOT at the end of surgery or after ICU admissions [19–21]. The reason for the inconsistent results might be the timing at which the VOT was performed. Microcirculatory alterations occur most severely during CPB via complex mechanisms, including hemodilution, production of free radicals, hypothermia, low flow, low pressure, non-pulsatile perfusion, and ischemia/reperfusion injuries [30,31]. However, the microcirculatory system has microvascular reactivity to recruit capillary reserves, wherein 70% of the capillaries can be opened under stress conditions [32,33]. If the patient has sufficient microvascular reactivity to compensate for the microcirculatory alterations induced by CPB, tissue hypoxemia would be minimized. If not, the tissue hypoxemia progresses, leading to poor clinical outcomes. Another reason the recovery slope during the CPB period was chosen as the primary outcome was the difference in perfusion pressure or oxygen delivery, which might influence the VOT parameters, making it easier to observe true microvascular reactivity.
In our study, the microcirculatory alterations progressively deteriorated from the induction of anesthesia until the CPB period, following a slow recovery after weaning from CPB. The differences in the VOT recovery slopes between patients with and without MAE might be progressively smaller, as the microcirculatory alterations are restored after weaning from CPB. Similarly, the AUROC for MAE predictions of the recovery slope at T4 was 0.637, which was less accurate than that of T2 or T3. No significant differences were seen in the AUROCs between them, and the specific point wherein the microvascular reactivity was the best MAE predictor could not be pinpointed.
Another notable point in this study was that the maximum StO2 values differed significantly between the patients with and without MAE throughout the study period. The maximum StO2 reveals hyperemic areas, which are also representative of microvascular reactivity. However, the maximum StO2 value was 95% in most cases, which is the upper limit of the INVOSTM measurement range [34]. Because of this ‘ceiling effect,’ the level of hyperoxygenation remained uncertain, potentially limiting the reliability of microvascular reactivity assessment. On the other hand, the recovery slope more accurately reflects the microvascular reactivity as compared to the maximum StO2 value, because the maximum StO2 is divided by the time taken regardless of a ceiling effect.
The knowledge and prediction of the postoperative outcomes is best obtained as early as possible to ensure the application of appropriate pre- or intraoperative preventive strategies. Moreover, the preventive strategies should be applied to select patients. Unfortunately, till date, the strategies to protect microcirculation are still under debate, with insufficient clinical evidence. Therefore, even if the prediction of postoperative outcomes is possible at early stages, there is currently a limit to improving the postoperative outcomes. Rather, accurate hemodynamic therapy for microcirculation protection, including precise fluid resuscitation and adjustment of organ perfusion pressure should be applied [35]. Importantly, they must be guided by microcirculatory monitoring, such as NIRS, side-stream or incident dark-field imaging, or peripheral perfusion index [35,36]. Additionally, the implementation of preventive strategies is desirable only in the high-risk groups. Implementing the preventive strategies in all patients is not feasible because the necessary tests or treatments can be delayed and are cost intensive.
Post-CPB vasoplegia is a common complication of on-pump cardiac surgery, with an estimated incidence of 5–25% [37]. Inflammatory mediators released during cardiac surgery result in the derangement of vascular reactivity [38]. A recent study showed that endothelial glycocalyx alterations after CPB were associated with postoperative vasoplegia in the CBP-treated patients [39]. In our study, the patients with MAE experienced post-CPB vasoplegia more frequently. The incidence of post-CPB vasoplegia did not differ between the patients with recovery slopes slope ≤1.08%/s at T2, which may be partially explained by the limited statistical power of the study.
In addition to the recovery slope at T2, additional factors like the hemoglobin at T1, duration of CPB, VIS at T3, and intraoperative urine output were also selected as risk factors for MAE in the multivariate regression model. Preoperative anemia is a well-known risk factor for postoperative complications in cardiac surgery [40]. Anemia may compromise the oxygen delivery, leading to tissue hypoxemia and increased pRBC transfusion, also an independent risk factor [41]. A longer CPB duration leads to longer exposure to inflammatory mediators, longer tissue hypoperfusion, higher risk of coagulopathy, and requirement for transfusion support [42]. A previous study showed that intraoperative inotropic therapy is associated with increased mortality and major postoperative morbidity after cardiac surgery [43]. The higher VIS after weaning from CPB may be related to the higher incidence of post-CPB vasoplegia in our study. A few studies have demonstrated that the urine output during CPB is associated with CSA-AKI [44]. In our study, only three patients had oliguria. Therefore, the clinical influence of intraoperative urine output on postoperative MAE remains unclear.
There are some limitations of the interpretation of our study results. First, INVOSTM was used to perform the VOT in our study. Our results are not comparable to those of previous studies that used InSpectraTM because of inter-device differences [34]. The baseline StO2 value was lower, and the recovery and occlusion slopes during VOT were faster on INVOSTM than on InSpectraTM. Second, the VOT was performed only once at the beginning of the CPB period. According to previous studies, the recovery slope progressively decreases during CPB and starts to increase after weaning from CPB [18,45]. In our study, the recovery slope at 10 min post-protamine injection was also a reliable predictor for MAE development. However, we assume that the VOT variables at this time point should be interpreted cautiously because the protamine may affect microcirculatory reactivity. Considering that microcirculatory disturbances may occur most severely during the CPB period, we cannot exclude the possibility that the recovery slope measured at the end of the CPB period may have been a better predictor.
In conclusion, our study demonstrated that the recovery slope of VOT during CPB could predict the occurrence of MAE post-cardiac surgery. Additionally, the patients with a lower recovery slope during CPB had higher SOFA scores and longer durations of ventilator care. These results support those of previous studies that showed that the disturbances in microcirculation induced by CPB can predict poor clinical outcomes. Furthermore, the results highlight the potential role of microvascular reactivity as an early predictor of MAE after cardiac surgery.