Gupta et al. [1] recently conducted an interesting meta-analysis on the comparative characteristics of video laryngoscopy (VL) compared to direct laryngoscopy (DL) for nasotracheal intubation (NTI) in oromaxillofacial surgeries.
This well-conducted meta-analysis of randomized controlled trials included data from 10 studies and showed that VL had significant advantages in terms of time to intubation (TTI) (mean difference, −9.04 s) and first-attempt success rate (SR) (relative risk [RR] 1.10) and required fewer maneuvers to facilitate intubation (RR 0.22). No differences were detected between VL and DL in terms of the overall intubation SR or incidence of nasal bleeding. The authors concluded that VL should be considered over DL for NTI in oromaxillofacial surgeries.
In order to assess the robustness of these findings, a trial sequential analysis (TSA) of the investigated outcomes is warranted before drawing strong conclusions in support of VL. Conducting a TSA helps to reduce the risks of type I statistical errors by providing evidence of the required information size (sample of patients needed) for the reported outcomes.
We used TSA Software (Copenhagen Trial Unit’s TSA Software®, Denmark) to perform the analysis. The information size was computed assuming an alpha risk of 5% with a power of 80%. We used a random-effects model and for the estimated effects on the investigated outcomes, we used the mean difference reported by Gupta et al. [1] for the continuous outcomes and RR reduction for dichotomous outcomes. Further details on TSAs and their interpretation are available elsewhere [2,3].
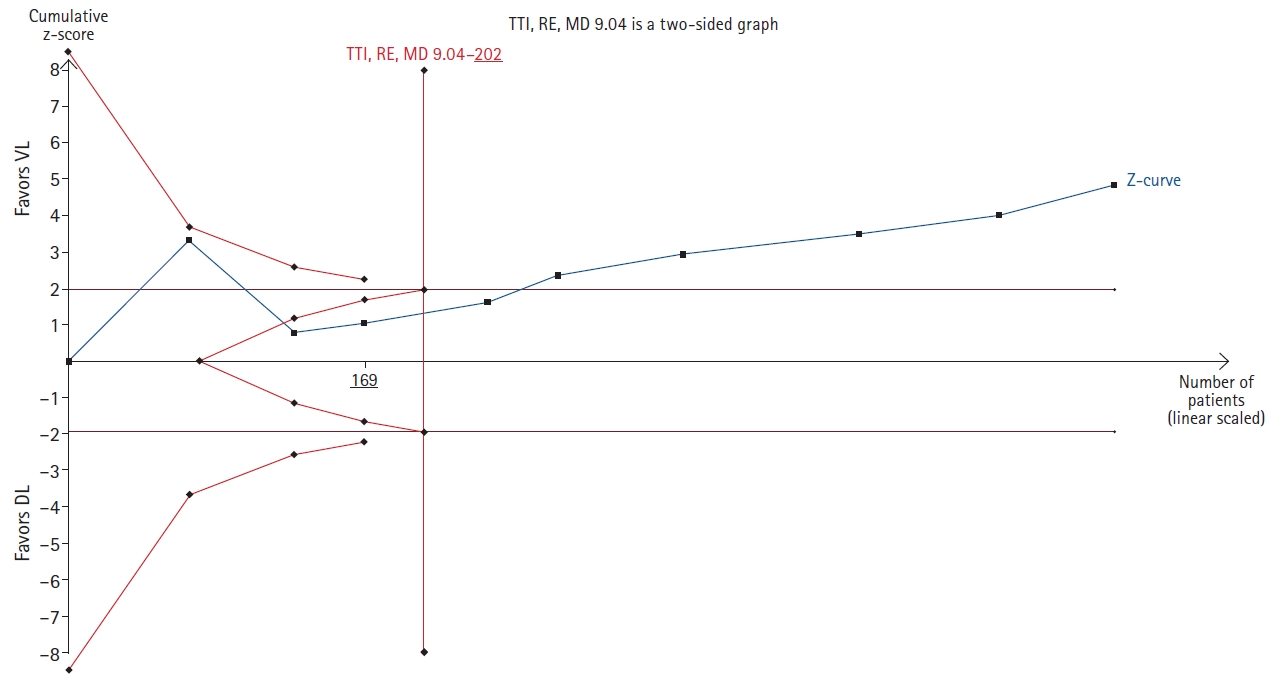
We conducted three TSAs in total to investigate the robustness of the study’s finding that VL is superior to DL for NTI in terms of TTI and first-attempt SR and to compare the number of maneuvers required for intubation. The TSAs showed that the required information size (or sample size needed) was achieved for all three outcomes, with a ratio of patients recruited/patients needed of 597/202 for TTI (Fig. 1), 467/263 for first-attempt SR, and 537/383 for the number of maneuvers required.
Importantly, all the TSAs conducted confirmed that the findings of Gupta et al. [1] were robust, as the Z-curve of effect crossed the adjusted significance thresholds for all the analyses.
In summary, while the authors conducted a scrupulous meta-analysis, performing a TSA is necessary to confirm the robustness of the investigated outcomes and to provide further support for the use of VL over DL for NTI in oromaxillofacial surgeries.