Obesity and anesthetic pharmacology: simulation of target-controlled infusion models of propofol and remifentanil
Article information

Abstract
The prevalence of obesity is increasing, resulting in an increase in the number of surgeries performed to treat obesity and diseases induced by obesity. The associated comorbidities as well as the pharmacokinetic and pharmacodynamic changes that occur in obese patients make it difficult to control the appropriate dose of anesthetic agents. Factors that affect pharmacokinetic changes include the increase in adipose tissue, lean body weight, extracellular fluid, and cardiac output associated with obesity. These physiological and body compositional changes cause changes in the pharmacokinetic and pharmacodynamic parameters. The increased central volume of distribution and alterations in the clearance of drugs affect the plasma concentration of propofol and remifentanil in the obese population. Additionally, obesity can affect pharmacodynamic properties, such as the 50% of maximal effective concentration and the effect-site equilibration rate constant (ke0). Conducting a simulation of target-controlled infusions based on pharmacokinetic and pharmacodynamic models that include patients that are obese can help clinicians better understand the pharmacokinetic and pharmacodynamic changes of anesthetic drugs associated with this population.
Introduction
The prevalence of obesity is increasing annually worldwide. According to the WHO report [1], 13% of the world’s adult population is obese, and the number has been growing steadily. In 2016, obesity was approximately three times what it was in 1975. In particular, the morbidly obese population, with a body mass index (BMI) > 40 kg/m2, is on the rise. Given the increase in the number of surgeries performed to treat obesity and associated diseases and the comorbidities present in this population, anesthesiologists are having an increasingly difficult time managing these patients. During surgery, anesthesiologists may have trouble with intubation and airway management before and after surgery, mechanical ventilation, control of diabetes and hypertension, obstructive sleep apnea, and cardiopulmonary disease.
In addition, pharmacokinetic and pharmacodynamic changes of anesthetic drugs in obese patients make it difficult to control the appropriate dose of anesthetic agents. The increase in body mass and changes of its composition influences pharmacokinetic parameters such as distribution volume, clearance, and elimination half-life. Comorbidities in obese patients, such as obstructive sleep apnea, may also cause narrowing of the therapeutic dynamic range of anesthetic drugs.
This review will include a discussion about the changes in various anesthetic drugs’ pharmacokinetic and pharmacodynamic behaviors that result from the increase in body mass and compositional changes that occur in obese patients based on published articles.
Changes in body mass composition
In obese individuals, the lean body mass, which includes vessel-rich organs and the tissues where drugs act, does not usually increase proportionally to the increase in total body mass. Rather, as the body weight increases, the blood volume, fat mass, lean body mass, and extracellular water volume increase along with the increase in total body weight (TBW); however, the composition of the mass does not always increase in proportion to the total body mass. The fat mass tends to increase along with the TBW; however, lean body mass does not. The ratio of lean body weight (LBW) to TBW decreases as the TBW increases. The proportion of LBW, which explains the increase in TBW, is approximately 20%–40% [2].
When a drug dosage is determined, it is usually scaled based on the TBW. However, administering drugs scaled simply using the TBW in obese patients would result in an overdose. Therefore, obese individuals need other mass scalars to calculate the appropriate dose, such as LBW, ideal body weight (IBW), and fat-free mass. Various mass scalars have been introduced, each with their own characteristic features and equations (Table 1).

Common Dosing Scalars
Total body weight
Dosing based on the TBW is valid for people with a normal weight. In obese patients, however, the lean tissue, which is where most cardiac output is delivered, does not increase in proportion to the TBW; therefore, the use of the TBW to determine the dose in obese patients would result in an overdose. Other mass scalars must therefore be considered.
Ideal body weight
Numerous equations have been introduced to calculate the IBW [3]. The disadvantage of this mass scalar is that individuals who have the same sex and height receive the same dose regardless of obesity and body mass composition.
Lean body weight
The LBW is the body mass without fat or adipose tissue. For the past several decades, James’ equation has frequently been used to calculate the LBW [4]; however, it has serious limitations for the obese population. The equation underestimates the LBW of morbidly obese individuals and even yields a flawed negative LBW. In 2005, Janmahasatian et al. [5] suggested another equation be used to overcome the limitations of James’ formula. This equation is derived from dual-energy X-ray absorptiometry measured in men and women of various body weights and heights. Most metabolic activities occur in the lean body mass, and an increase in cardiac output is closely correlated with an increase in the LBW. Therefore, the early distribution kinetics of the drug and clearance are influenced by cardiac output.
Adjusted body weight
The adjusted body weight (ABW) is defined as the IBW plus a proportion (40%) of the excess TBW compared to the IBW. The ABW is calculated as the IBW + 0.4 × (TBW – IBW).
Body mass index
The BMI is widely used to determine the degree of obesity and is calculated as the ratio of the body weight (kg) to the height (m) squared. However, the BMI does not consider the body mass composition.
Body surface area
The body surface area (BSA) has been primarily used as a dosing scalar for chemotherapeutic agents. The equations derived by Mosteller [6] are widely used. However, the BSA does not discriminate between fat and lean body mass.
Pharmacokinetic mass
Due to the non-linear relationship between fentanyl clearance and the TBW, if fentanyl was administered based on the TBW, obese patients would be overdosed. Shibutani et al. [7] therefore devised a modified weight called pharmacokinetic mass, in which the mass scalar increases in proportion to the increase in clearance. The ‘pharmacokinetic mass’ is reported to be highly correlated with the LBW.
Allometric scaling
Allometric scaling is a method that establishes a relationship between the body mass and pharmacokinetic or pharmacodynamic parameters with a certain fixed exponent constant α, calculated as follows: Clearance = β × (TBW)α. Alpha is usually called the allometric coefficient. Allometric scaling is designed to apply animal experiment results to humans or to assume pediatric doses from adult data [8–10]. Allometric scaling can sometimes be useful in determining the drug dosages for obese patients. However, extrapolating analyzed data out of the range, such as data from non-obese to obese populations, has inherent problems.
Changes in pharmacokinetic properties
The various physiological and anthropometric changes that occur in obese patients affect pharmacokinetic parameters, such as distribution volume and clearance, which are used to determine drug concentration and dosage. The characteristic changes in patients with obesity that affect pharmacokinetic parameters, which are not present for those with a normal weight, include an increase in lean body mass, muscle mass, fat mass, circulatory blood volume, and total body water. In addition, changes in the lipophilicity or hydrophilicity and protein binding of drugs affect pharmacokinetic parameters in obese patients [11,12].
The increase in fat mass associated with obesity increases the distribution volume of lipophilic drugs [13-15]. In a study of thiopental, which has high lipophilicity, the steady-state distribution volume and the elimination half-life in obese patients was found be considerably higher. [16]. A study of propofol also showed that the volume of distribution increases in proportion to the increase in the TBW [17]. While the volume of distribution of this lipophilic drug does increase as fat mass increases, it does not increase proportionally. The reason for this is related to changes in blood flow to the adipose tissue, which accounts for 5% of cardiac output in non-obese patients, but it is reduced to 2% in obese patients [18].
The increase in the central volume of distribution associated with obese individuals leads to a rapid decrease in concentration during the initial distribution phase. The loading dose is mainly determined by the size of the central volume of distribution, which determines the changes in the initial concentration after administration. In addition, the increase in cardiac output, which is a commonly observed physiological change in obese patients, is another factor explaining low plasma concentrations in the distributive period [19,20].
Increased cardiac output plays an important role in the increase in the overall clearance of drugs, thus lowering the elimination half-life of the drug. The increase in cardiac output in patients with obesity is highly correlated with the increase in the LBW [21,22]. Increased cardiac output and increased LBW are associated with increased renal and hepatic blood flow, which in turn increase the overall clearance and initial distributive clearance [23,24].
The increase in cholesterol levels and free fatty acids in obese patients has been found to inhibit the binding of drugs to plasma proteins, such as albumin. There is also a disagreement, however, as binding of the drug to plasma proteins increases due to increased levels of α-acid glycoproteins in obese patients [25-28].
Changes of pharmacodynamic properties
Excess fat caused by obesity leads to disturbances in body metabolism and inflammatory reactions and increases drug sensitivity [29,30]. Some studies have shown that obesity increases pain sensitivity, while other studies have found no adverse or pharmacodynamic effects [31-33]. Cortinez et al. [34] did not find any changes in the pharmacodynamic parameters in obese patients. Dong et al. [35], however, reported a decrease in the 50% of maximal effective concentration in obese patients and an increased sensitivity to propofol.
Considering that obesity affects both pharmacokinetics and pharmacodynamics, determining the dose of propofol based on the EEG processed monitor (e.g., BIS, entropy) should be considered. Subramani et al. [36] reported that the induction dose of propofol based on the BIS index was different from the induction dose based on LBW in morbid obese patients. In this study, compared to the amount of propofol administered based on the LBW, a larger amount was administered when the dose was based on the BIS. These authors also reported that for those who were administered propofol based on the LBW, 60% of them required an additional dose of propofol to obtain a sufficient depth of anesthesia. The Eleveld model also suggests that the effect-site equilibration rate constant (ke0) changes as the body weight changes, using the equation 0.146 × (weight [kg] / 70)-0.25.
Target-controlled infusion model for the obese population
Studies on a target-controlled infusion (TCI) model for the obese population have been conducted using several drugs, including propofol and remifentanil [37-42]. If the obese population was not included in the process of building a TCI model and not equipped into the anesthetic delivery pump, the exact target effect concentration cannot be obtained by calculating doses simply based on the TBW of an obese patient.
However, some reports have stated that changing the weight scalar of the known TCI model to something other than the TBW improves the performance of the model in obese patients. Cortinez et al. [43] reported an improvement in the performance of the TCI model by simply switching the original weight scalar with an alternative weight scalar. They stated that the performances of the Shnider and Marsh models were dramatically improved after substituting the TBW with the ABW. La Colla et al. [40] proposed using a fictitious height, or an adjusted height, for the Minto model to offset the inaccurate influence of the LBW when the model is applied to obese individuals.
However, these types of proposed shortcuts are not a definitive solution. Constructing a new pharmacokinetic model that includes data obtained from obese patients would be a more desirable approach. Eleveld et al. [44] and Kim et al. [42] presented integrative models for propofol and remifentanil, respectively, by gathering data from various pharmacokinetic studies that included obese patients.
Simulations
Before administering drugs to obese patients, simulations based on pharmacokinetic or pharmacodynamic models are helpful for planning drug administration. A simulation model that includes the obese population would help clinicians discover unexpected errors and prepare for them in advance. Therefore, the Eleveld and Kim models were simulated to discover the differences in the pharmacokinetics of propofol and remifentanil between obese and non-obese individuals.
It is clinically impractical to administer propofol and remifentanil independently at each target concentration without consideration of the interaction. The interaction between propofol and remifentanil, therefore, should be considered in the simulation of obese patients. The target concentration of propofol and remifentanil should be adjusted to reflect a real clinical situation in which an interaction of the drugs occurs.
For this interaction, the hierarchical model proposed by Bouillon et al. [45] was referenced. The target concentration for induction and maintenance of anesthesia was maintained at the target concentration combinations of the two drugs, achieving a rate of 95% no response to laryngoscope intubation or hypnosis (Fig. 1). The resultant predicted concentration of each drug simulated by the scenario is plotted in Fig. 2.
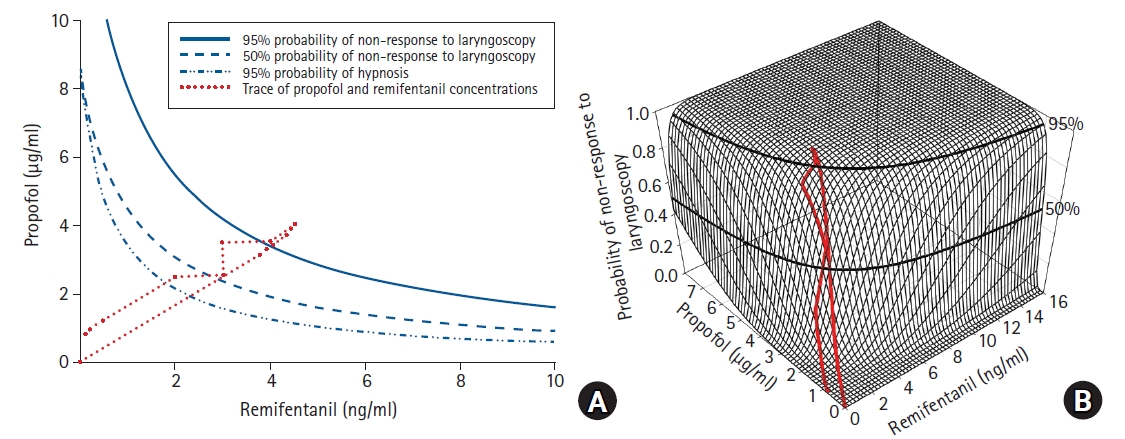
Planning of the simulation based on loss of responsiveness predictions. (A) Isoboles are presented on top-down view. Isoboles of 95% and 50% non-response to laryngoscope and hypnosis are presented. The inward bow of the isoboles indicates that the interaction is synergistic. (B) Simulated target concentrations are plotted on the interaction surface.

Resultant effect-site concentrations of propofol and remifentanil. Target concentration of propofol and remifentanil are predicted according to the simulated scenario.
The Eleveld and Schnider models were compared for the propofol simulation, while the Minto and Kim models were compared for the remifentanil simulation. In the Eleveld model, various covariates are used to determine the pharmacokinetic and pharmacodynamic parameters. These covariates include the coadministration of opioids and the participant’s health status (patient or healthy volunteer), among others. While all cases could not be covered by this simulation, the influences of weight and age were simulated. A simulation was performed for a healthy volunteer who was administered an opioid and remifentanil and was 170 cm in height. The ke0 from the Minto model was used as a reference for the Kim model, since it does not include the ke0. The purpose of the simulation was to show the changes in the total cumulative dose and infusion rate according to various BMIs and ages.
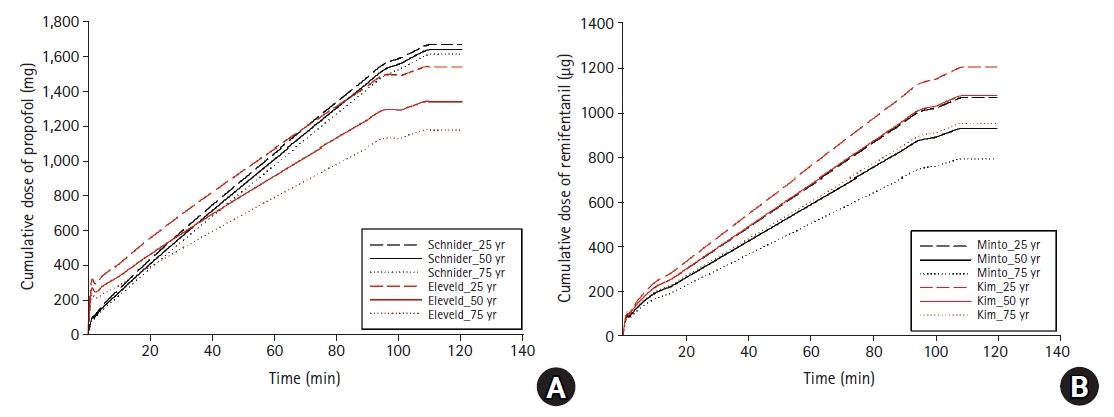
The cumulative dose of the Eleveld model was larger than that of the Schnider model early in the TCI. This was because the Schnider model has a small and fixed central compartment volume, while the Eleveld model has a relatively larger central compartment volume, which requires a relatively larger amount of propofol at the beginning of the TCI to maintain the same target concentration (Fig. 3A).

Comparison of distribution volumes and clearance. Central volumes of distribution and clearance are compared between the pharmacokinetic models by changing the BMI. (A) Central volume of distribution changes in propofol models, (B) Clearance changes in propofol models, (C) Central volume of distribution changes in remifentanil models, (D) Clearance changes in remifentanil models. BMI: body mass index.
Later in the TCI infusion, however, the cumulative dose of the Schnider model was found to increase more than that of the Eleveld model. As the BMI increased, however, the clearance of the Schnider model increased much more than that of the Eleveld model (Fig. 3B). The explanation for this finding is that with a relatively high clearance, a higher dose of the drug is needed to maintain the same target concentration. This trend was significantly more prominent in obese than in non-obese individuals (Fig. 4A). Therefore, when TCI is performed with the same target concentration, the initial infusion rate of the Eleveld model was faster but gradually decreased over time since the clearance was lower than that of the Schnider model (Fig. 4B).

Comparison of cumulative doses and infusion rates. The cumulative doses and infusion rates are presented by altering the BMI, at a fixed age of 50 years. (A) Cumulative doses of propofol models, (B) Infusion rates of propofol models, (C) Cumulative doses of remifentanil models, (D) Infusion rates of remifentanil models. BMI: body mass index.
When the Minto and Kim models for remifentanil were compared for people with a normal BMI, the central compartment volume and clearance did not appear to be different between the models. However, as the BMI increased, the central compartment volume and clearance according to the Minto model did not increase in proportion to the BMI because the LBW of James’ equation was installed in every parameter of the Minto model. In James’ equation, LBW decreases with increasing body weight in morbidly obese individuals (Fig. 3C). However, the central compartment volume and clearance using the Kim model increased according to the increase in the BMI. The Kim model does not use James’ equation but rather applies the fat-free mass from the Janmahasatian equation, which is used to calculate the fast-peripheral compartment volume. The central compartment volume and clearance with the Kim model are generally predicted to be larger than those with the Minto model. As the BMI increased, the difference in the central compartment volume and clearance between the two models increased (Fig. 3D). Therefore, when a TCI is performed using the Kim model, the cumulative dose is predicted to be larger over time than that using the Minto model. The difference in the cumulative dose between the two models was larger in obese patients (Fig. 4C). The infusion rate was also higher in the Kim model, but both models showed similar trends throughout the simulation (Fig. 4D).
An additional simulation considering the influence of age showed that the difference in the cumulative dose of propofol between the models increased with age. In the case of remifentanil, however, the difference in the cumulative dose between the two models remained constant for all age groups (Fig. 5).
Comparison of the cumulative doses. The cumulative doses are presented by varying the age, with a fixed BMI of 45 kg/m2. (A) Cumulative doses of the propofol models, (B) Cumulative doses of the remifentanil models. BMI: body mass index.
Discussion
Regardless of applying an appropriate mass scalar for induction and maintenance of anesthesia, the target concentration cannot be guaranteed by manual administration using a simple calculation of the dose. In other words, a holistic TCI device equipped with an appropriate pharmacokinetic and pharmacodynamic model is needed to control the concentration of anesthetic drugs. Drug infusions through the TCI system is theoretically the most accurate and fastest way to reach the target concentration, but it requires an accurate model to support it. Many pharmacokinetic and pharmacodynamic models, however, were created from data that did not include information of obese patients, and therefore cannot accurately predict concentrations of drug in blood in these patients. Recently, a few models have been introduced that can be applied to both obese patients and general patients [42,44].
The Eleveld model is a well-constructed model that can be used to administer more accurate concentrations of drugs to individual patients through the inclusion of various covariates relevant to actual clinical situations. Since the Eleveld model includes the use of opioids as a covariate, among others, this model may be a more practical model. When propofol is administered in clinical practice, opioids such as remifentanil are almost always administered together, and the two drugs may affect each other pharmacokinetically and/or pharmacodynamically [46]. The propofol simulation conducted for this review also included covariates for opioid use to reflect the effect of co-administration of remifentanil.
Based on the Eleveld model, the central compartment volume does not increase significantly (16.2%) with an increase in BMI. The clearance of obese patients, however, increases as the BMI or weight increases (54.9%). Clinically, this means that if propofol is administered to obese patients during anesthesia induction with a bolus dose based on the TBW, an overdose may occur because of relatively small increase of central compartment volume. In the case of continuous infusions, however, TBW could be adopted as a dosing scalar for anesthesia even for obese patient as the clearance of obese patient increase enough with the increase of TBW [17,34]. These observations are consistent with previous reports which have found that the increase in the volume of distribution is relatively small while the increase in clearance is prominent in obese [18,23,24].
Even though the best model can accurately predict concentrations, it cannot take all clinical situations into account. Pharmacokinetic changes in propofol can be influenced by various factors, such as very lean or underweight body types, laparoscopic surgery, and a prone posture [47-50]. Propofol itself can cause pharmacokinetic changes. The cardiac depression caused by propofol affects its own distribution and clearance. Therefore, rather than trying to discover every variable that may affect pharmacokinetics and create endless new models, it is essential that patients monitoring, such as the BIS, be used to confirm whether the purpose of the drug is achieved.
However, how many models are currently available for TCIs? Most commercial infusion pumps are not equipped with the new models that have been built for obese patients. To apply a new TCI model suitable for obese patients, an infusion pump must be connected to a computer with TCI software, through which a pharmacokinetic/pharmacodynamic model suitable for obese patients can be run. Another method is to apply an appropriately modified scalar instead of using the patient’s actual height or weight in the model already installed in a commercial TCI pump. Through using the ABW instead of the TBW for the traditional Schnider and Marsh models, or inputting a fictitious height for the Minto model, replacing true patient data is a possible solution; however, modified scalars are not a perfect solution.
In conclusion, simply administering an anesthetic drug based on body weight to obese patients is associated with a high risk of overdosing. Comorbidities associated with obesity can further increase the risk of overdosing. To determine the appropriate dose for obese patients, it is important to understand how the pharmacokinetics and pharmacodynamics change as the body weight increases. Factors that affect the pharmacokinetic changes in obese individuals include an increase in adipose tissue, LBW, extracellular fluid, and cardiac output.
Several mass scalars, including the IBW and LBW, have been introduced to more appropriately calculate drug dosages for obese patients; however, there are no mass scalars that can be applied to all drugs and individuals. Therefore, it is important to carefully monitor the effects and side effects of the drugs during administration.
Notes
Funding
This work was supported by a 2-year Research Grant from the Pusan National University (201911630003).
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.