Introduction
The target-controlled infusion (TCI) system allows for intravenous administration of anesthetic agents with a pump by incorporating pharmacokinetic models [1]. Users can control target plasma concentration (Cp) or effect-site concentration (Ce) of propofol using a TCI system. Currently, only the modified Marsh and Schnider pharmacokinetic models are used for propofol in commercially available TCI pumps [2,3,4,5]. In general, as Ce represents the effect of propofol, the target Ce-controlled infusion is more commonly used than the target Cp-controlled infusion during anesthesia using propofol [6].
In general, adults with a body mass index (BMI) of less than 18.5 kg/m2 are defined as underweight according to the World Health Organization [7]. Crohn's disease is an inflammatory condition involving the gut, with consequent absorption disorders found in 70% of the patients. Malnutrition has been reported in 65–75% of patients with Crohn's disease [8], and subsequent weight loss is common [9]. In our clinical experience, administration of propofol and remifentanil using target Ce-controlled infusion with the modified Marsh and Minto models was associated with insufficient anesthesia in underweight patients with Crohn's disease [3,10,11]. Additional administration of midazolam was required to maintain bispectral index (BIS™ Covidien, Boulder, CO, USA) values at less than 60 during anesthesia induction and maintenance, compared to conventional anesthetic dosing strategies employed at our hospital. Although external validation studies previously demonstrated that the modified Marsh and Schnider models were clinically acceptable [12,13], the predictive performance of these two models has not been evaluated in underweight patients.
The aim of this retrospective study was to compare the clinical performance of the modified Marsh model for propofol between underweight and normal-weight patients with Crohn's disease, before evaluating the predictive performance of the modified Marsh and Schnider pharmacokinetic models in underweight patients.
Materials and Methods
Dosing strategies for propofol and remifentanil using TCI
We retrospectively reviewed the medical records of 50 patients who underwent elective surgery for Crohn's disease at our hospital. The Institutional Review Board of the Asan Medical Center approved this retrospective review (approval number: 2016-1327). The anesthetic dosing strategies employed in these patients were as follows. Two milligrams of midazolam was administered intravenously prior to propofol infusion, and additional midazolam was administered to maintain BIS values at less than 60 during induction and maintenance of anesthesia if necessary. Patients received long-chain triglyceride (LCT) propofol (Pofol®, Jeil Pharmaceutical, Seoul, Korea) via target Ce-controlled infusion using the modified Marsh model [3,10], whereas remifentanil was administered via target Ce-controlled infusion using the Minto model [11]. Propofol and remifentanil were infused using the Asan Pump TCI software (version 2.1.3, Bionet, Seoul, Korea, http://www.fit4nm.org/download, last accessed: Aug 27, 2012), and the infusion profiles for all patients were automatically recorded in a .csv file format. Target Ce values of propofol were adjusted within a range of 2.5–3 µg/ml to maintain BIS values at less than 60 during anesthesia maintenance. Target Ce values of remifentanil were titrated within a range of 3–20 ng/ml to maintain stable hemodynamics (systolic blood pressure > 80 mmHg and heart rate > 45 beats/min).
Simulations
The infusion profiles of the patients were used as input to the Schnider model [14]. Simulations were performed using the Asan Pump software to calculate the simulated Ce of the Schnider model. Deterministic simulations, which considered neither inter-individual nor intra-individual random variability, were performed. Clearance, as calculated by the modified Marsh and Schnider models according to the changes in body weight, was simulated in a hypothetical underweight patient. The effects of height, age, weight, and sex on propofol clearance were compared using simulation in the Schnider model. The pharmacokinetic parameters and blood-brain equilibration rate constant (ke0) for the modified Marsh and Schnider models are presented in Table 1 [2,3,4,5].
Data collection
Demographic data of patients, duration of anesthesia, and total doses of midazolam, propofol, and remifentanil were collected. Mean infusion rates of propofol and remifentanil were calculated by dividing the total anesthetic agent dosages by body weight and anesthesia maintenance time. In addition, Crohn's disease activity index (CDAI) was calculated [15].
Statistical analyses
Statistical analyses were conducted using R (version 3.1.2, R Foundation for Statistical Computing, Vienna, Austria) or SigmaStat version 3.5 for Windows (Systat Software, Chicago, IL, USA). Data were expressed as mean ± SD for normally distributed continuous variables, medians (25–75%) for non-normally distributed continuous variables, and numbers and percentages for categorical variables. P values of less than 0.05 were considered statistically significant for all analyses.
Results
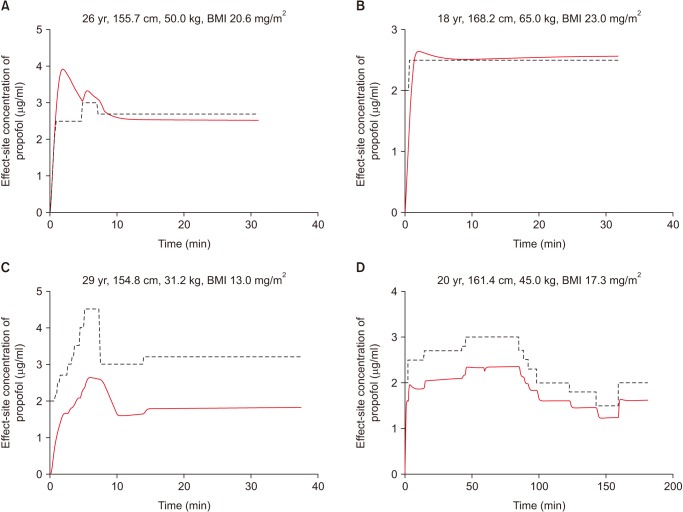
Demographic and clinical characteristics of the patients and the dosages of anesthetic agents administered during surgery are shown in Table 2. The total midazolam and remifentanil amounts required for underweight patients were larger than those required for normal-weight patients, indicating that the target propofol range of 2.5–3 µg/ml determined by the modified Marsh model is insufficient to satisfy the anesthetic requirement in underweight patients. This assumption was supported by a simulation study based on the Schnider model, which used the infusion profile of propofol administered via target Ce-controlled infusion based on the modified Marsh model (Fig. 1). The differences in Ce values at identical time points between the Schnider and the modified Marsh models were larger among underweight patients. Specifically, the Ce values of the Schnider model were consistently lower than those of the modified Marsh model.
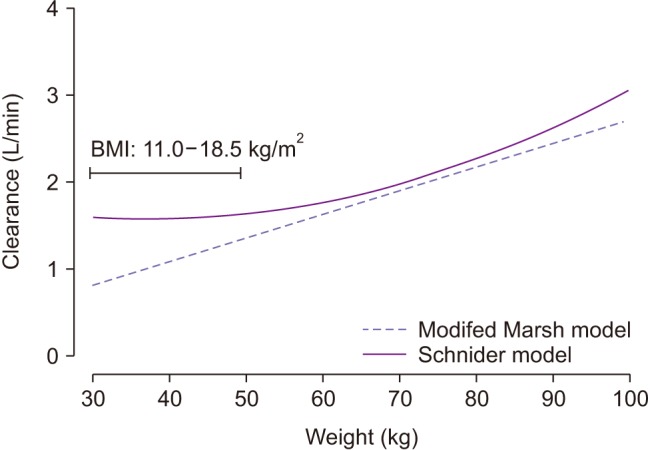
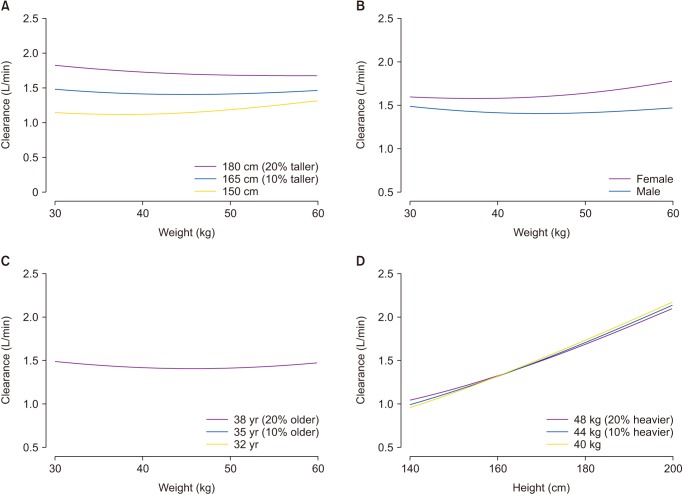
The simulated clearances, which were based on changes in weight using the modified Marsh and Schnider models, are shown in Fig. 2. The propofol clearance was consistently higher in the Schnider model than in the modified Marsh model, particularly in subjects with a BMI of less than 18.5 kg/m2. A simulation showing the effects of height, age, weight, and sex on propofol clearance using the Schnider model is shown in Fig. 3. Female sex as well as 10% and 20% increases in height led to marked increases in propofol clearance using the Schnider model, whereas 10% and 20% increases in age and weight resulted in minor changes.
Discussion
In the current study, a dosing strategy established by a previous study was utilized to adjust target Ce values of propofol within a range of 2.5–3 µg/ml and to maintain BIS values at less than 60 [16]. The mean (SD) Ce associated with a 95% probability of loss of consciousness (Ce95) was 2.22 (0.44) µg/ml for LCT propofol [16]. In addition, the response surface model demonstrated the additive effects of propofol and remifentanil on BIS [17]. In particular, remifentanil concentrations greater than 4 ng/ml significantly reduced the propofol concentration required to blunt the response to a noxious stimulus [17]. Based on these findings, target Ce values of propofol were titrated within a range of 2.5–3 µg/ml in the clinical setting.
In general, low body weight simply indicates that a person's weight is low, whereas the definition of underweight usually applies to a person whose weight is low for their height. The modified Marsh model includes body weight as the only covariate that significantly affects the volume of distribution in the central compartment [10]. In contrast, height, lean body mass, body weight, and age are all included as covariates in the Schnider model [4]. In particular, height, lean body mass, and body weight are significant covariates for clearance, which is an important pharmacokinetic parameter for determining the rate of infusion to maintain a target concentration:
where Css is the steady-state drug concentration in plasma. As depicted in Fig. 2, the discrepancy of Ce between the Schnider and the modified Marsh models in underweight patients can be explained by differences in clearance.
Sex, age, height, and weight of hypothetical persons were used as covariates to evaluate their influence on the amount of propofol required to maintain a certain Ce level. The simulation showed that the clearance of propofol was positively associated with increasing height as well as with female sex (Fig. 3). In particular, height was the most significant covariate in determining the amount of propofol required to maintain a target Ce.
A fundamental limitation of the current study was its retrospective design. Several confounding factors including Crohn's disease severity and concurrent medications could affect the results of the current study. Crohn's disease severity is commonly evaluated using CDAI [15]. CDAI values were 286.5 ± 101.2 and 252.4 ± 76.3 for the underweight and normal-weight patient groups, respectively (P = 0.302). Additionally, concurrent medications in the current cohort, which included sulfasalazine, azathioprine, methotrexate, cyclosporine A, tacrolimus, and mercaptopurine, did not differ significantly between the underweight and normal-weight patients with Crohn's disease. Furthermore, there were no significant differences in laboratory parameters including aspartate transaminase, alanine transaminase, alkaline phosphatase, serum albumin, and total bilirubin between the two groups. Despite the presence of many covariates that could affect the findings in the current cohort, the simulation results explained the cause of higher dosage requirements for midazolam and remifentanil in underweight patients receiving propofol via target Ce-controlled infusion using the modified Marsh model. This finding highlights the necessity of clinical research to evaluate the predictive performance of the modified Marsh and Schnider pharmacokinetic models in underweight patients.
In conclusion, the total midazolam and remifentanil dosages required for underweight patients were higher than those required for normal-weight patients to maintain BIS values at less than 60 within a target propofol Ce range of 2.5–3 µg/ml. This finding suggested that the utilization of the modified Marsh model caused inadvertent propofol underdosing in underweight patients. Simulation results suggested that the Schnider model may be an appropriate pharmacokinetic model for TCI in underweight patients, as the propofol clearance in the Schnider model was consistently higher than that in the modified Marsh model, particularly in underweight patients. Future studies are necessary to compare the predictive performance of the modified Marsh and Schnider pharmacokinetic models in underweight patients.