Acute coronary syndrome (ACS) is a rare complication associated with infective endocarditis (IE) [1]. Vegetation may cause direct occlusion of the coronary artery, especially in the case of aortic valve (AV) vegetation. The anesthesiologist should consider the possibility of coronary compression due to coronary embolism or obstruction of the coronary ostium due to the vegetation, and both the left and the right coronary ostia should be checked via transesophageal echocardiography (TEE) [2] when the patients with IE present acute hemodynamic disturbance, sign of ACS, or myocardial ischemia. Intraoperative TEE is a valuable tool for the evaluation of vegetation size and location. We report a case of a left main coronary artery ostium occlusion in an infective endocarditis, with transesophageal image.
Case Report
A 43-year-old woman, with no significant previous medical history, was admitted due to fever, chills, and headache which she had been experiencing for the past several days. Her laboratory work showed a cell count of 20 /µl with 38% neutrophils on cerebrospinal fluid analysis, and elevated levels of serum troponin I (11.59 ng/ml) and creatine kinase-MB (17.6 ng/ml). Her transthoracic echocardiography (TTE) showed severe rheumatic aortic stenosis (AS) with mild aortic regurgitation (AR) and a normal left ventricular (LV) systolic function. We needed a complete TEE for further evaluation, but the patient refused the examination. Eventually, a diagnosis of infective endocarditis was made via TTE finding with clinical correlation. When the patient was admitted, an antibiotic therapy was performed for the control of infection. Brain magnetic resonance imaging showed multiple embolic infarctions in the frontal, parietal lobe and left corpus callosum. There were Janeway lesions on her both feet. After 5 days of antibiotic treatment under the suspicion of IE, subsequent atrial flutter and acute pulmonary edema developed. Serum troponin I (48.14 ng/ml) and creatine kinase-MB (81.3 ng/ml) were elevated more compared to the results at the admission. An emergent aortic valvuloplasty was decided.
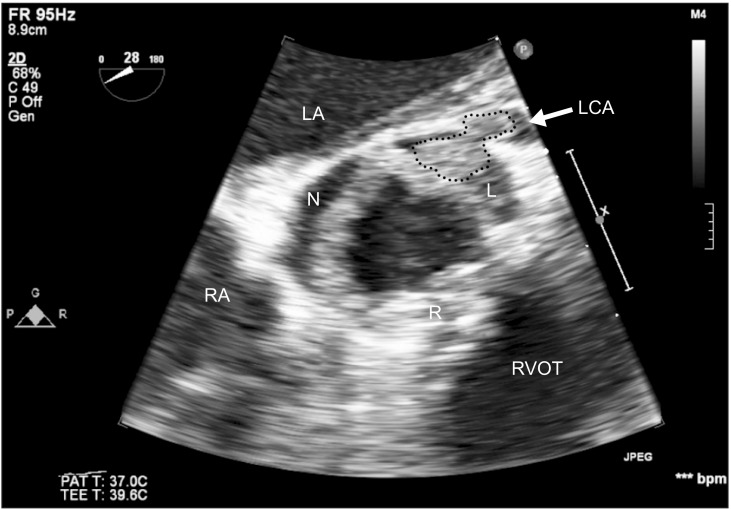
Intraoperative TEE examination confirmed severe AS and relatively fresh 1.5 cm vegetation on LCC of the AV with frequent diastolic prolapse into the aortic root (Fig. 1). This mobile vegetation partially occluded left coronary ostium (Fig. 2), but it did not cause cardiac failure; the ejection fraction (EF) was 55 % by modified Simpson's method. The right coronary ostium was not occluded by the mobile vegetation. TEE showed the vegetation to be in good position across the AV (Video 1 and 2). There was no regional wall motion abnormality (RWMA) in intraoperative TEE.
The surgeon confirmed the state of AV as severe commissural fusion, severe thickening with relatively fresh 1.5 cm vegetation, and left coronary ostium partial occlusion by the vegetation. The AV replacement with removal of vegetation and mitral valvuloplasty was performed. The patient was weaned from CPB without any hemodynamic instability or changes in ST segment on electrocardiography (ECG).
The patient's cardiac output was 4.0-5.4 L/min and cardiac index was 2.3-3.1 L/min/m2, and there was no change in ST segment of 12-lead ECG immediately after the operation in the intensive care unit. The cardiologist confirmed well-functioning of prosthetic mechanical AV and akinesia of apical cap with normal LV EF (59%) via TTE. She was discharged on the 28th postoperative day without any complication.
Discussion
ACS is a rare complication associated with IE [1]. Nonetheless, the anesthesiologist should consider the possibility of coronary compression due to periannular aortic valve abscess and pseudoaneurysms, and coronary embolism or obstruction of the coronary ostium due to the vegetation, to be able to make the diagnosis using TEE when the patients with IE present acute hemodynamic disturbance, sign of ACS, or myocardial ischemia.
The patient in this study could have been diagnosed as ACS, because of the angina, high serum troponin I (48.14 ng/ml), and creatine kinase-MB (81.3 ng/ml) occurring during the early phase. However, there was no evidence of RWMA in the intraoperative TEE. We assumed that the vegetation prolapsed into the left coconary ostium, and that it induced a partial occlusion of the left coronary ostium and a spontaneous escape of the vegetation from the ostium.
The major echocardiographic findings for the diagnosis of IE are vegetation, abscess, and new dehiscence of prosthetic valve. The vegetation is the most important lesion for the diagnosis of IE, and an oscillating mass attached to valvular structure is a typical characteristic of vegetation. Another major echocardiographic finding for endocarditis is the perivalvular abscess, which is presented by reduced echo density without color flow detected inside [3]. The patient was diagnosed as IE due to presence of the oscillating vegetation on AV, but there was no abscess formation.
Vegetation may cause direct occlusion of the coronary artery, especially in the case of AV vegetation. The anesthesiologist should check both the left and right coronary ostia via midesophageal (ME) short-axis view of the aortic valve, and the right coronary ostium via an ME long-axis view [2].
Coronary embolism is another mechanism for myocardial ischemia in patients with IE. There are several causes of the coronary embolism [4]. Intraoperative TEE is a valuable tool for the evaluation of vegetation size and location. If the vegetation is large (> 10 mm) and movable or fragile, it can increase the incidence of embolism.
Another cause of coronary embolism is LV mural thrombi which can be seen in a spontaneous echo contrast. Spontaneous echo contrast is definitive sign of slackened blood flow which is considered as a prothrombotic condition. A thrombus shows well-defined margins and discrete echo dense mass throughout systole and diastole. There are other embolic sources such as cardiac tumors, especially the valvular tumors. Echocardiographic contrast perfusion imaging may be useful in confirming the vascularity of cardiac masses and in differentiating the vascular tumors from benign tumors and thrombi.
In the rare cases of myocardial ischemia associated with coronary obstruction due to the vegetation in IE patients, echocardiographic findings may present a new RWMA, although there was no RWMA in our case.
The TEE is helpful for finding the etiology in the patient with IE, who is presented with ACS, and the management of the complication can be different according to the mechanisms. Furthermore, the intraoperative TEE could present the unknown or new lesions that were not discovered by the preoperative TTE, although the new findings from TEE may not affect the method of the operation.