Introduction
Total intravenous anesthesia (TIVA) has the merit of rapid and predictable emergence from anesthesia. However, the rapid offset of short-acting intravenous agents, while desirable, may incur inadequate postoperative analgesia. Thus, active intervention and careful transition from intraoperative to postoperative analgesia must be established. Fentanyl is a common opiate for postoperative analgesia, and its minimum effective plasma concentration (Cp) was reported as 0.63 ng/ml, ranging from 0.23 to 1.18 ng/ml [1]. The primary hyperalgesia due to skin incision was reported to subside within 1 hr, but the secondary hyperalgesia was known to develop maximally within 30 min and persist for 3 hr [2]. Furthermore, various studies on the postoperative analgesia using intravenous fentanyl show that postoperative pain scores remains high until 4 or 6 hr postoperatively [3-9].
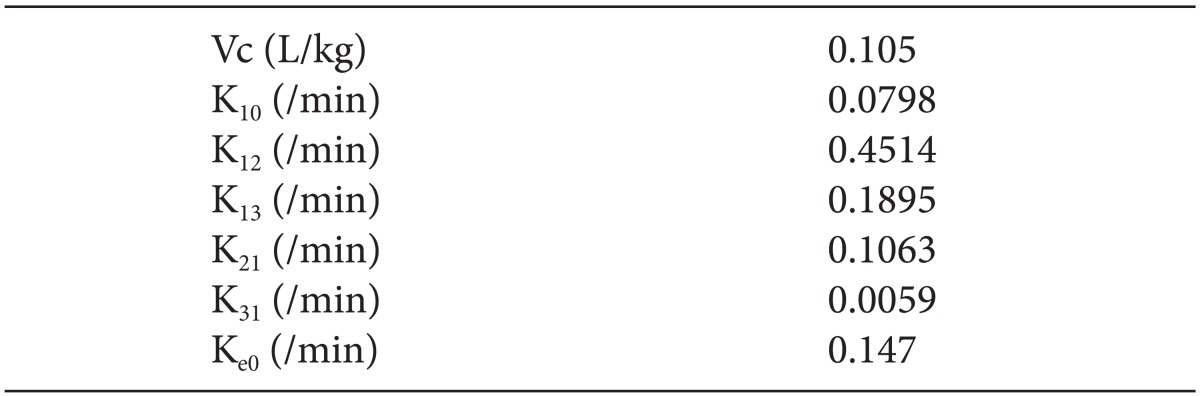
Intravenous postoperative pain management, using short-acting opiates, usually involves a continuous background infusion, and a patient-controlled analgesia (PCA). However, the pharmacokinetic/pharmacodynamic (PK/PD) simulations of fentanyl, using the PK/PD software (STANMUMP©, SL Shafer, Department of Anesthesia, Columbia University, New York, NY, USA) with the weight-scaled three-compartment PK model [10] and the effect-site compartment [11,12] (Table 1), showed delayed increases to a steady-state of the effect-site concentration (Ceff) during various fixed-amount infusions following 1.0 µg/kg of initial bolus, which were more predominant at lower rate background infusions (Fig. 1). Therefore, the analgesic concentration in the body might be insufficient to the severity of the early postoperative pain during the fixed-rate infusion of the recommended regimens (< 1.1 µg/kg/hr) [1,5,7,13,14]. But fixed-set to higher rates (1.25-2.0 µg/kg/hr) [6,13] might increase the risk of side effects, such as ventilatory depression, while 50% depressing the slope of the ventilation-CO2 response curve at the Cp of fentanyl between 2.0-3.1 ng/ml [15].
Therefore, we established time-scheduled decremental background infusions of fentanyl, which were programmed to cope with the time course of postoperative analgesia after propofol/remifentanil-based TIVA, and their efficacy and safety were compared with those of the fixed-rate background infusion.
Materials and Methods
This study was approved by the Institutional Review Board and written informed consent was obtained from all patients. A total of 99 female patients of American Society of Anesthesiologists physical status 1-2 and aged 20-65 years, who wanted postoperative pain management after laparoscopic-assisted hysterectomy, were enrolled in this study. Exclusion criteria included a history of neurologic, psychiatric, endocrinologic, renal or hepatic disorders. Drug or alcoholic abusers and patients taking analgesics or sedatives were also excluded. The instructions of pain control device and the expression method of the pain intensity were explained at the pre-anesthetic visit.
The anesthetic technique of TIVA was standardized. As a premedication, glycopyrrolate 0.2 mg was administered intravenously, but no sedatives and opiates were given. Routine monitoring consisted of electrocardiograph, pulse oximetry, non-invasive arterial pressure, end-tidal carbon dioxide partial pressure, and bispectral index (BIS). TIVA was induced using propofol (Fresofol®, Fresenius Kabi, Homburg, Germany) and remifentanil (Ultiva™, GlaxoSmithKline, Rixensart, Belgium) target-controlled infusions (TCI), which were administered using two-channel infusion pump (Orchestra®, Fresenius Vial, Brezins, France) with corresponding PK/PD models [16,17]. For neuromuscular blockade, 0.6 mg/kg of rocuronium was given by IV. After tracheal intubation, propofol and remifentanil TCIs were titrated to maintain BIS of between 40-60, and systolic blood pressure and heart rate as ± 20% of baseline values. Any patient who needed to receive opiates and analgesics other than remifentanil was designed to be excluded from this study. Single intravenous palonosetron 0.075 mg was administered after the induction of anesthesia to prevent the postoperative nausea and vomiting (PONV) [18]. Postoperative pain management was prepared during surgery and performed at the end of TIVA, as follows.
A balloon-type, disposable infuser (Auto-Fusor®, AceMedical Corp., Ltd, Seoul, Korea), which had a module for PCA and a basal infusion rate controller (AutoSelector®, AceMedical Corp., Ltd, Seoul, Korea), was filled with 100 ml of fentanyl diluent (Fentanyl citrate®, Hana Pharm. Co., Seoul, Korea), which was prepared by an anesthesiologist who was otherwise not involved in the postoperative pain assessment. According to body weight, individual fentanyl diluent was made to be equivalent to 0.25 µg/kg of fentanyl per 1.0 ml of diluent, using normal saline. During the surgery, the infuser and its extension lines were primed while diluent was evacuated to atmosphere. When the skin closure started, propofol/remifentanil TCI stopped. Thereafter, fentanyl diluent 4 ml (= 1.0 µg/kg) was injected during 30 s [19], when the Ceff of remifentanil TCI decreased to 2.0 ng/ml [20]. The infuser was connected at the proximal portion of the indwelling cannula of the patient using three-way stopcock, and an anti-reflux one-way valve was inserted to prevent the backflow to the gravity infusion line for anticipating an occlusion.
Patients were randomized to one of the three groups (FX2-2-2, D6-4-2 and D8-4-2) consisting of 33 patients in each group, using Excel© 'Random' function (Microsoft Office® Excel 2007). In FX2-2-2, the background infusion rate was maintained at a fixed-rate of 2.0 ml/hr until postoperative 24 hr, without changing the infusion rate [5,7]. In decremental infusion groups, the infusion rates were maintained at 6.0 ml/hr (D6-4-2) and 8.0 ml/hr (D8-4-2) until postoperative 1 hr, respectively, and decreased to maintain at 4.0 ml/hr during postoperative 1-3 hr. Thereafter, they were decreased to 2.0 ml/hr during postoperative 3-24 hr (Fig. 1). PCA bolus amount was 1.0 ml (= 0.25 µg/kg) with 15 min of filling time. When the patients opened their eyes, deep breathing was encouraged, and extubation was done, after the reversal of residual neuromuscular blockage using glycopyrrolate 0.4 µg/kg and pyridostigmine 0.2 mg/kg. The patient was then transported to the postanesthesia care unit (PACU).
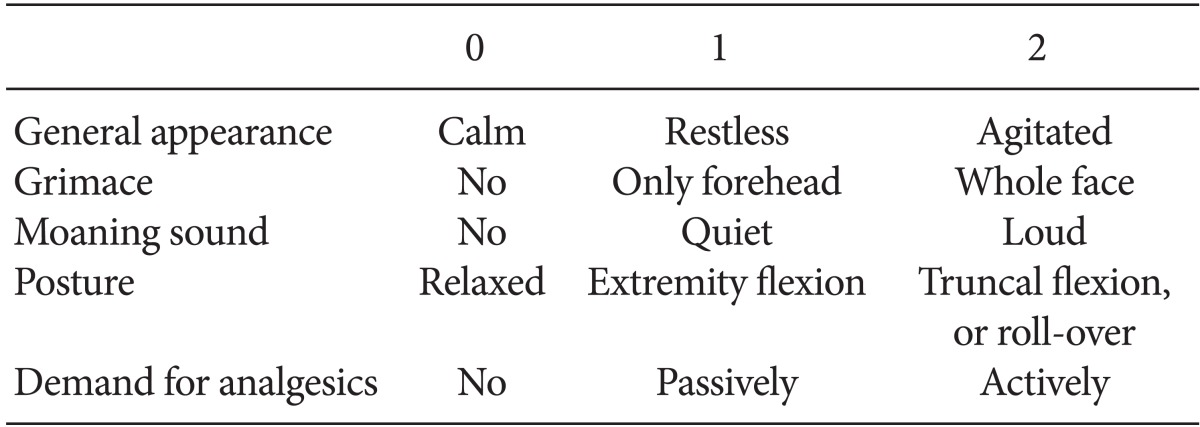
Routine monitoring was implemented at PACU, and the Aldrete three-point postanesthesia recovery score that assessed five areas (activity, respiration, blood pressure, color, and level of consciousness) was measured at 5-min intervals [21]. The efficacy of analgesia was assessed both subjectively and objectively, at 15 min interval: (i) Patient was asked to state a graded visual analogue scale (VAS, at rest, no pain = 0, the worst possible pain = 10), subjectively. (ii) An investigator, blinded to the group allocation, evaluated the analgesia using 'Observer's Objective assessment of pain scores' (OOAPS) (Table 2). The total up of the five areas' scores was defined as OOAPS. The primary efficacy measures of this study included 'inadequate analgesia' in the PACU, which was defined to be at least one more episode of 'VAS > 3 or OOAPS > 0' at every 15 min-interval assessments of pain. When a patient showed inadequate analgesia, fentanyl diluent 1 ml (= 0.25 µg /kg) was administered using PCA module, and in case of inadequate analgesia at the final assessment of pain in the PACU, ketorolac 30 mg IV was given as a rescue analgesic. After one hour of PACU care, the patient who had obtained higher than 8 points of the recovery score was transported to the general ward. The patient was instructed to use PCA voluntarily in the ward and to record the time of PCA episode using lap-time memory of stopwatch. Ketorolac 30 mg iv was also administered as a rescue analgesic in the ward. The assessments of analgesia and patient condition were performed at the time points of postoperative 2, 3, 4, 6, 12 and 24 hr.
The following end points in the PACU and ward were examined: VAS change, PCA episode, rescue analgesics, alertness, ventilatory depression (respiration rate < 6 /min), bradycardia (heart rate < 20% of baseline), PONV, headache, and dizziness. The intensities of PONV were measured using a four-point categorical scale of 'none' to 'severe', and palonosetron 0.025 mg was administered as a rescue therapy according to the patient's request. When assuming the severe side effects of fentanyl, background infusions were reduced to 1.0 ml/hr. At the last visit of postoperative 24 hr, or at the time of withdrawal from the study, the satisfaction score on the overall postoperative pain management (based on an eleven-point categorical scale of '0 = worst' to '10 = best') was asked to the patient, and in case of dissatisfaction, the major reason for that was questioned. Post-hoc individual simulation of the time-course of Ceff of fentanyl was performed based on each background infusion rate and the recorded lap time of PCA demand, using the same PK/PD software described above.
For the calculation of the sample size, a pilot study was conducted for 30 patients given the bolus and background infusion same as this study, which showed 80.0% of 'inadequate analgesia' during 0.5 µg/kg/hr and 46.7% at 1.5 µg/kg/hr of background infusions in the PACU. To obtain a two-sided test of difference using α = 0.05 and β = 0.2, the sample size was estimated at 33 evaluation subjects per group.
Statistical analyses were executed using SPSS 10.0 for windows (SPSS Inc, Chicago, IL, USA). Data are expressed as mean ± SD or number of patients (%). Categorical variables were compared using chi-square, or Fisher's exact test, where appropriate. Repeated-measures ANOVA were used to compare VAS changes over time among the groups, followed by Duncan's post-hoc testing. Continuous variables between the groups were compared by using one-way ANOVA with Bonferroni post-hoc testing. Null hypotheses of no difference were rejected if P values were less than 0.05.
Results
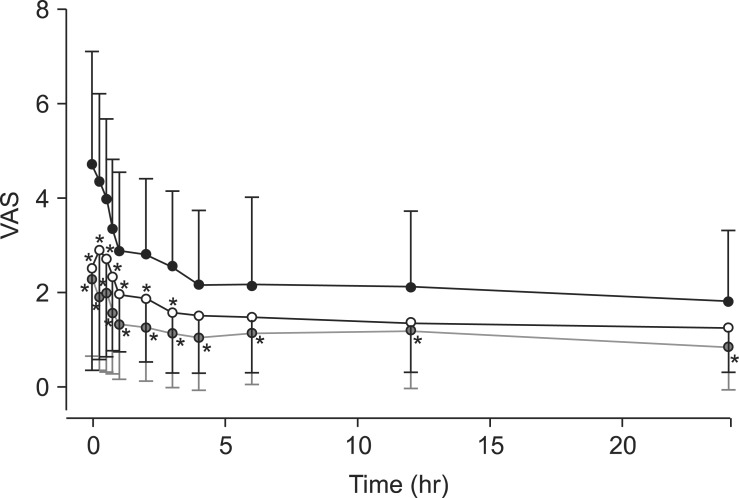
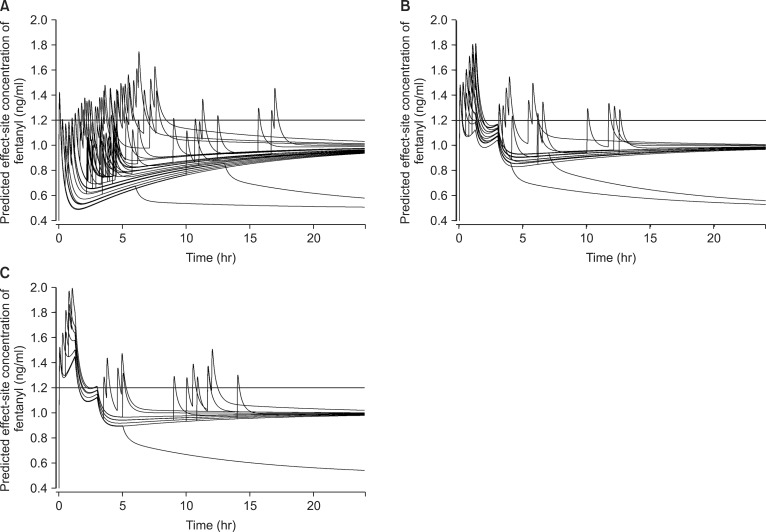
Patient characteristics including age, body weight, height, and the duration of surgery and anesthesia, had no statistically significant differences for patients among groups (Table 3). All ninety-nine patients completed the study with no withdrawal; however, the background infusions of 5 patients had to be decreased to 1 ml/hr at ward because of severe PONV. There were statistically significant within-group effects of time on the postoperative VAS change (P < 0.001). The difference in VAS over time was statistically significant between groups (P < 0.001) (Fig. 2). VAS was significantly higher in the FX2-2-2 group than in the D6-4-2 and D8-4-2 groups from immediate postoperative period to postoperative 3 hr (P < 0.05). After postoperative 4 hr, VAS was significantly higher in the FX2-2-2 group than in the D8-4-2 group (P < 0.05) (Fig. 2). Individual time courses of predicted Ceff are illustrated at Fig. 3. However each graph has not demonstrated 33 individual curves, because the subjects who had not used the PCA module were simulated to have the same time courses of Ceff.
Analgesic efficacy
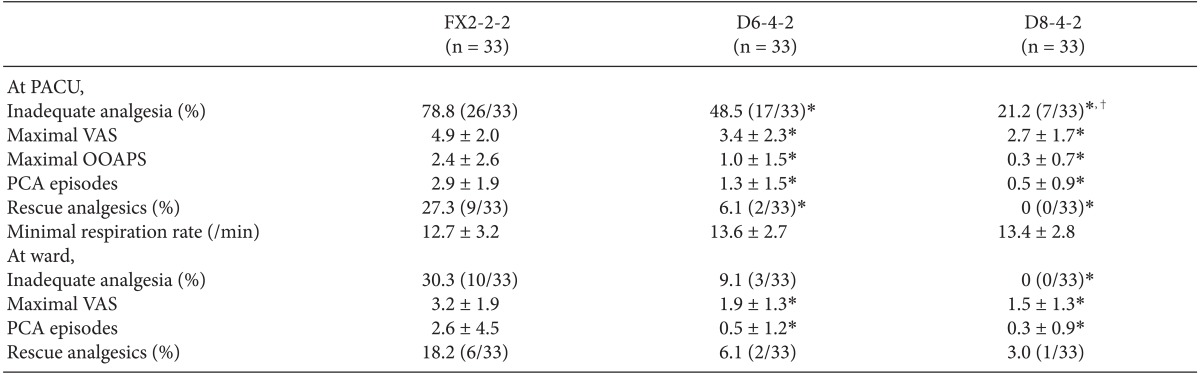
At PACU, the proportion of patients with inadequate analgesia of FX2-2-2 was significantly greater than the decremental infusion group of D6-4-2 (P = 0.038) and D8-4-2 (P < 0.001) (Table 4). The mean maximal VAS and the mean maximal OOAPS of FX2-2-2 were significantly higher than those of D6-4-2 and D8-4-2, and the mean episodes of additional fentanyl diluent using PCA bolus in FX2-2-2 was also greater than those of D6-4-2 and D8-4-2. The proportion of patients who required rescue analgesics in FX2-2-2 was greater than in D6-4-2 and D8-4-2. The highest VAS was 9, 7, 7 and the highest OOAPS was 9, 5, 3 in FX2-2-2, D6-4-2 and D8-4-2, respectively.
In the ward, compared with the fixed-rate infusion group of FX2-2-2, the proportion of patients with inadequate analgesia was greater than D6-4-2, but statistically not significant (P = 0.06). However, the proportion of inadequate analgesia of D8-4-2 was smaller than that of FX2-2-2 (P = 0.001) (Table 4). The maximal VAS and PCA episodes of FX2-2-2 were significantly greater than those of D6-4-2 and D8-4-2, but the proportion of patients who were administered rescue analgesics were not different among groups. The highest VAS in the ward was 7 in FX2-2-2, and 4 in both D6-4-2 and D8-4-2.
Safety and side effects
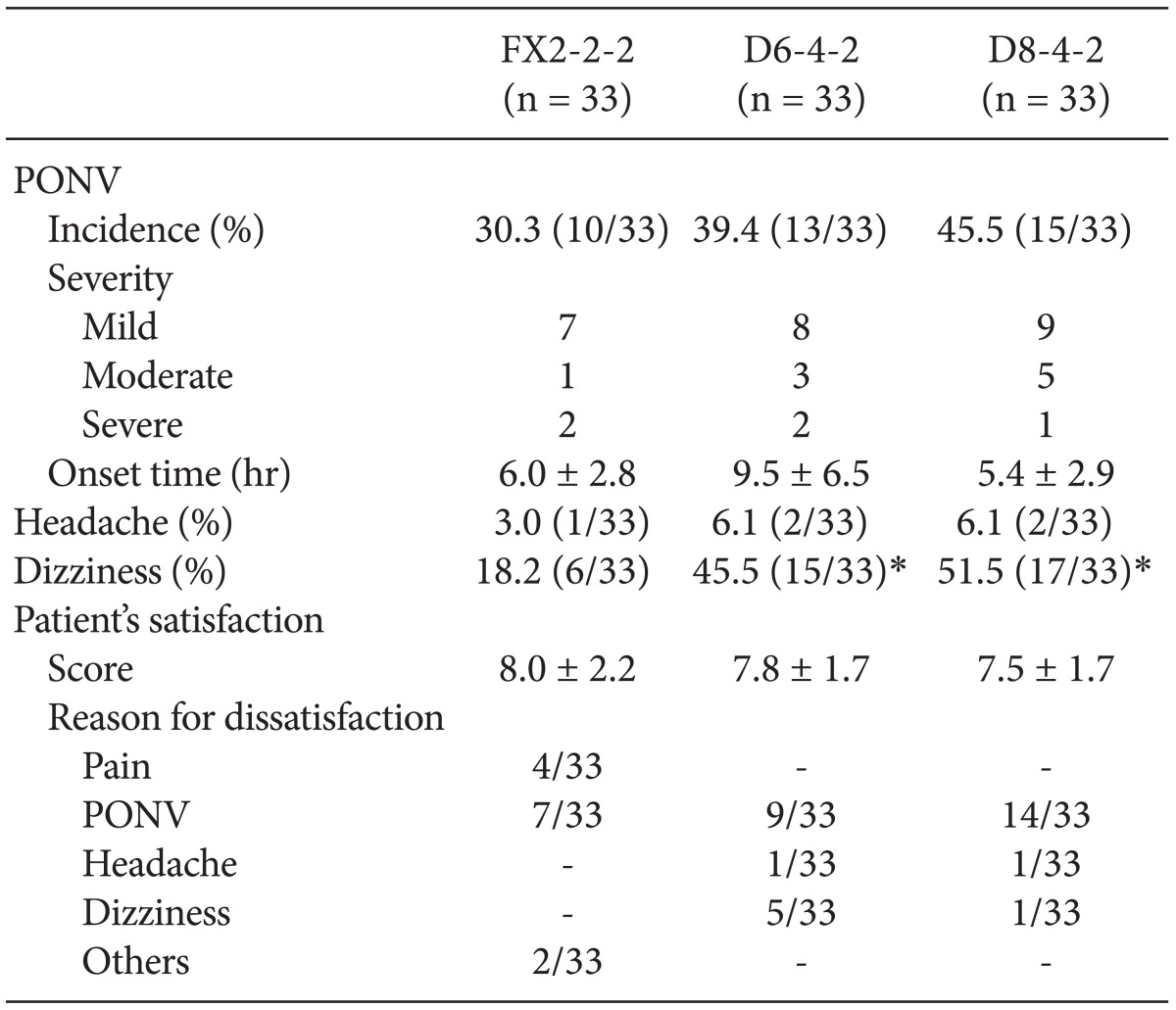
The minimal respiration rates in the PACU were not significantly different among groups, and no patient showed ventilatory depression in the PACU and ward (Table 4). The occurrence and the onset time of PONV were not different among groups (Table 5). No patient showed PONV at PACU, but 5 patients developed severe PONV, and their background infusion rate had to be decreased to 1 ml/hr at ward. The incidence of headache also did not differ significantly among groups, but the incidence of dizziness in FX2-2-2 was lower than in the decremental groups.
Patient satisfaction
The levels of patient satisfaction were not different among groups. The reasons for dissatisfaction were in most cases complaint of incomplete postoperative analgesia, PONV and on economic grounds (e.g. high cost) in FX2-2-2. On the contrary, in the decremental infusion groups, most of the dissatisfaction was from PONV.
Discussion
The regimen of the time-scheduled decremental background infusions of fentanyl for the postoperative analgesia after propofol/remifentanil-based TIVA has been demonstrated to provide less inadequate analgesia and less PCA intervention than the fixed-rate background infusion, especially in the early postoperative period. In addition, no regimens resulted in ventilatory depression, and were not significantly different in terms of PONV.
Some studies have found that concurrent background infusion of morphine was not superior to the sole PCA module for the postoperative analgesia [22,23]. On the contrary, with PCA, using short-acting fentanyl alone to maintain adequate analgesia, over 70% of patients required several re-adjustments to the PCA settings or supplemental boluses, compared to only 20% of patients during morphine PCA [3]. The background infusion with fentanyl PCA was considered to be necessary for effective analgesia. However, recent studies evaluating the effectiveness of postoperative analgesia using the concomitant background infusion of fentanyl, still had not provided reliable adequate analgesia including PCA bolus and a background infusion [3-9]. Accordingly, we tried to establish the infusion method while varying the infusion rates of the diluents. Along with the result of the preliminary study, to decrease the incidence of the inadequate analgesia over 20% at the immediate postoperative period, the initial infusion rates had to be maintained three times higher (> 1.5 µg/kg/hr) than the previously reported infusion rate (0.5 µg/kg/hr). Hence, the initial infusion rates were chosen as 1.5 and 2.0 µg/kg/hr. However, the rationale for these faster infusion rates might be inferred by the pharmacokinetics of fentanyl, as well as the nature of postoperative pain. The PK simulation of intravenous fentanyl showed that Cp and Ceff rapidly increased following a bolus injection, then decreased, however increased slowly during the constant zero-order infusions following a bolus injection (Fig. 1), and in order to rapidly increase the Cp and Ceff, a much faster infusion rate was needed. However, those faster infusions might increase the possibility of the occurrence of side effects, such as ventilatory depression. Thus, it was decided to decrease the infusion rates to 4 ml/hr and 2 ml/hr at the postoperative 1 hr and 3 hr as the simulated concentrations began to increase. The reason for this late increase of Cp of fentanyl might be considered the slow equilibrium of the peripheral compartments. During the TCI of fentanyl when the Cp at the central compartment is maintained at a constant level, the concentrations (C2 and C3) at the peripheral compartments become equal to Cp around at 40 min for C2, and 15.7 hr for C3.
VAS is a practical and familiar assessment of pain intensity during the management of postoperative pain. All patients were educated how to express the pain on the pre-anesthetic visit. In some cases, patients' exact self-reporting of the degree of the pain using VAS seemed to be questionable, even though they had fully awaken. Therefore, an additional scoring system of pain was introduced in this study for an objective assessment of pain intensity. The OOAPS used five-item scales, which were scored from 0 to 2. Each item was selected from the various pediatric postoperative behavioral pain rating scales [24-26], but the combination of the items of the OOAPS system in our study might reasonably be tested in further investigation as a potential scoring system during the immediate postoperative period.
The most dangerous side effect of opioids during the postoperative analgesia might be the respiratory depression. The background infusion amount of D8-4-2 was 4 times greater than the fixed-infusion group, but the gross inspection of the simulation graphs of the Ceff of fentanyl (Fig. 3) showed that Ceff hardly exceeded the 2.0 ng/ml of Ceff that had been reported to increase the incidence of ventilatory depression [15], and in D8-4-2 (Fig. 3C), the Ceff of fentanyl of two subjects after PCA boluses, approached to 2.0 ng/ml, but no case of respiration rate less than 6 /min was recorded during the period of PACU or ward. At PACU, the routine monitoring equipment might be sufficient to promptly detect and manage ventilatory adverse events, but vigilance is needed to prevent respiratory morbidity in the ward. In case of the accidental occlusion of intravenous infusion route during the long-term infusion at ward, the infusate would flow backward to the gravity line, and the accumulated large amount of fentanyl could be injected rapidly after occlusion release. There is no guarantee that this fatal incident would not take place, and various safety devices, such anti-reflux valve or alarm system, should to be considered.
The overall satisfaction scores on the management of analgesia did not differ significantly among groups. Four patients of FX2-2-2 had complained about the insufficiency of the pain management, while none of the decremental infusion groups had expressed their dissatisfaction on the analgesia. However, the major reason for dissatisfaction was PONV. The incidence of PONV was similar with the previously reported studies using the same prophylactic dose of palonosetron after inhalation anesthesia [18], and also have been reported as 45% using dexamethasone and ondansetron prophylaxis during intravenous fentanyl PCA [27], where the background infusion rate was 0.4 µg/kg/hr. The characteristics of the occurrence of PONV in our study as follows; First, it did not happen in the PACU, and this could have been due to the residual propofol which maintained subhypnotic low Cp during the stay in the PACU [28]. Second, the mean onset time of PONV were about the postoperative 5.4-9 hr. As such, we might anticipate that another downward regulation of background infusion would be helpful for the decrease of the incidence of PONV during fentanyl PCA. However, further research on the regulation time and infusion amount of the background infusion might be required.
There are some caveats to be discussed here. First, the most useful technique for intravenous infusion of opioids may be the TCI for the background infusion and PCA. But the commercially available opioid TCI, such as Remifusor® (Graseby 3500® with prototype Remifentanil TCI system, Smiths Medical International, Watford, UK), and various TCI pumps have limitations on use at ward and portability during ambulation. Further development and implementation of a small portable TCI-PCA device would be helpful to regulate the infusion rate automatically. Second, the decremental infusion regimens of this study could be also applied from the start of anesthesia using concurrent infusion of remifentanil or not, and beneficially need less intervention of medical personnel at the postoperative period. However, in case of the hemorrhage or hemodilution during surgery, the PK of fentanyl and the resulting prediction of analgesia might be altered [29]. Third, as previously reported [1], the infusion rate of fentanyl for analgesia showed wide range, inter-individual difference. About twenty percent of patients in FX2-2-2 had adequate analgesia, with predicted Cp of fentanyl maintained around 0.5 ng/ml during PACU, while about twenty patients in D8-4-2 needed supplemental PCA, with Cp was predicted to maintain above 1.3 ng/ml. Therefore, some challenge tests estimating the postoperative analgesic requirement will be helpful to select an appropriate background infusion rate at the initiation of the infusion diluents [30].
In conclusion, the time-scheduled decremental background infusions of fentanyl for postoperative analgesic management after TIVA could achieve more satisfactory analgesia and needed less PCA intervention of the patient and the medical personnel than the conventional fixed rate background infusion, without any increase of risk and side-effects.