-
Predictors and indicators
- Jong Yeon Park
-
Korean J Anesthesiol. 2024;77(2):173-174.
-
Editorial
March 13, 2024
|
-
 Anesthetic management for non-cardiac surgery in patients with left ventricular assist devices
Anesthetic management for non-cardiac surgery in patients with left ventricular assist devices
- Jeong-Jin Min, Yang Hyun Cho, Sangmin M. Lee, Jong-Hwan Lee
-
Korean J Anesthesiol. 2024;77(2):175-184.
-
Review Article
March 10, 2023
|
-
 The impact of preoperative coronavirus disease 19 infection on early postoperative mortality during the vaccination era: a nationwide retrospective cohort study
The impact of preoperative coronavirus disease 19 infection on early postoperative mortality during the vaccination era: a nationwide retrospective cohort study
- Jae-Woo Ju, Taeyup Kim, Soo-Hyuk Yoon, Won Ho Kim, Ho-Jin Lee
-
Korean J Anesthesiol. 2024;77(2):185-194.
-
Clinical Research Article
January 26, 2024
|
-
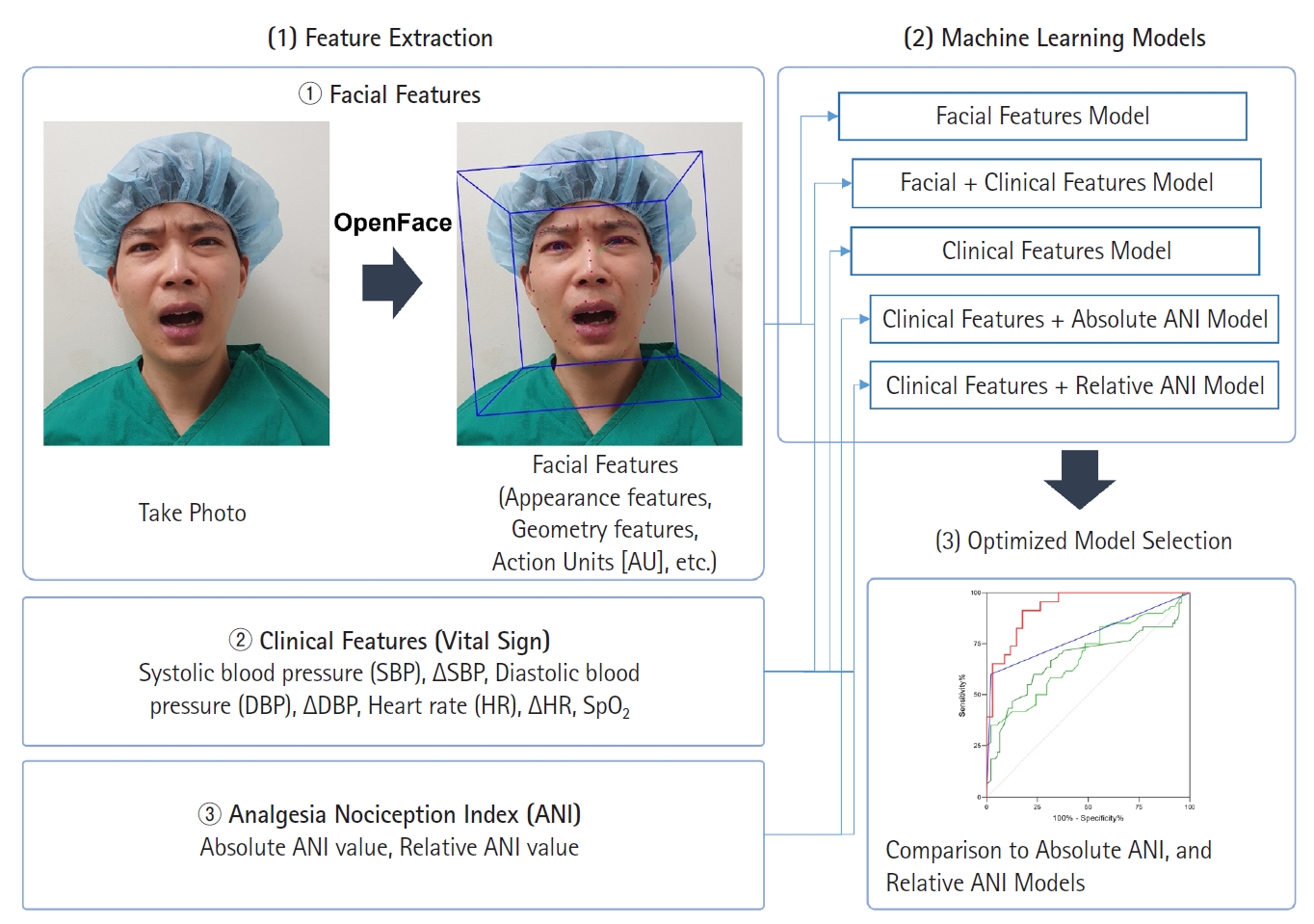 Machine learning model of facial expression outperforms models using analgesia nociception index and vital signs to predict postoperative pain intensity: a pilot study
Machine learning model of facial expression outperforms models using analgesia nociception index and vital signs to predict postoperative pain intensity: a pilot study
- Insun Park, Jae Hyon Park, Jongjin Yoon, Hyo-Seok Na, Ah-Young Oh, Junghee Ryu, Bon-Wook Koo
-
Korean J Anesthesiol. 2024;77(2):195-204.
-
Clinical Research Article
January 5, 2024
|
-
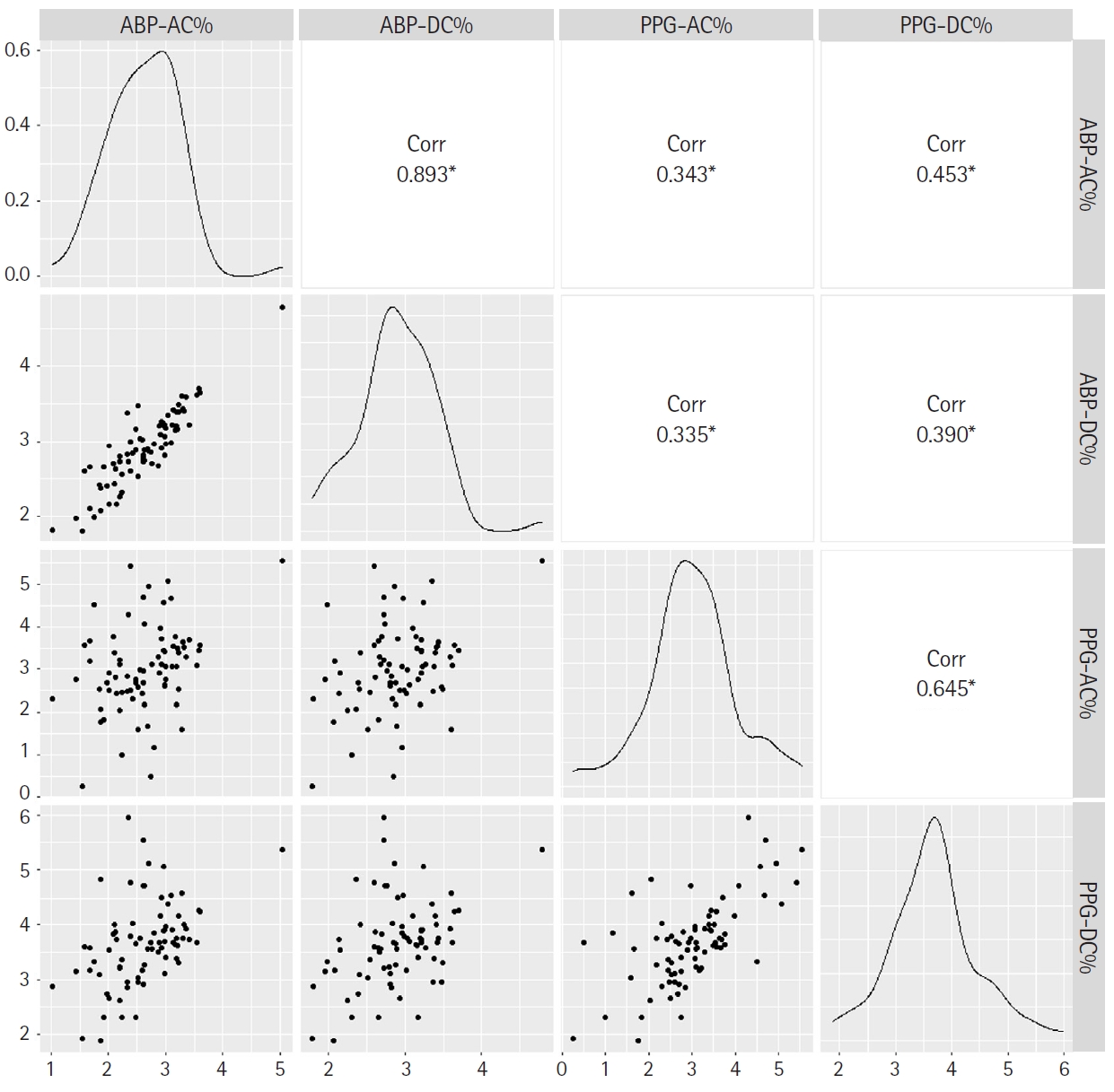 Frequency domain analysis of photoplethysmographic and arterial pressure waveforms for assessing hemodynamics in children with congenital heart surgery
Frequency domain analysis of photoplethysmographic and arterial pressure waveforms for assessing hemodynamics in children with congenital heart surgery
- Hwa-Young Jang, In-Kyung Song, Sung-Hoon Kim, Won-Jung Shin
-
Korean J Anesthesiol. 2024;77(2):205-216.
-
Clinical Research Article
January 11, 2024
|
-
 Postoperative alterations in ventriculoarterial coupling are an indicator of cardiovascular outcomes in liver transplant recipients
Postoperative alterations in ventriculoarterial coupling are an indicator of cardiovascular outcomes in liver transplant recipients
- Ji Yeon Kim, Young-Jin Moon, Changjin Lee, Jin Ho Kim, Junghyun Park, Jung-Won Kim
-
Korean J Anesthesiol. 2024;77(2):217-225.
-
Clinical Research Article
July 12, 2023
|
-
 Association of preoperative blood glucose level with delirium after non-cardiac surgery in diabetic patients
Association of preoperative blood glucose level with delirium after non-cardiac surgery in diabetic patients
- Soo Jung Park, Ah Ran Oh, Jong-Hwan Lee, Kwangmo Yang, Jungchan Park
-
Korean J Anesthesiol. 2024;77(2):226-235.
-
Clinical Research Article
January 4, 2024
|
-
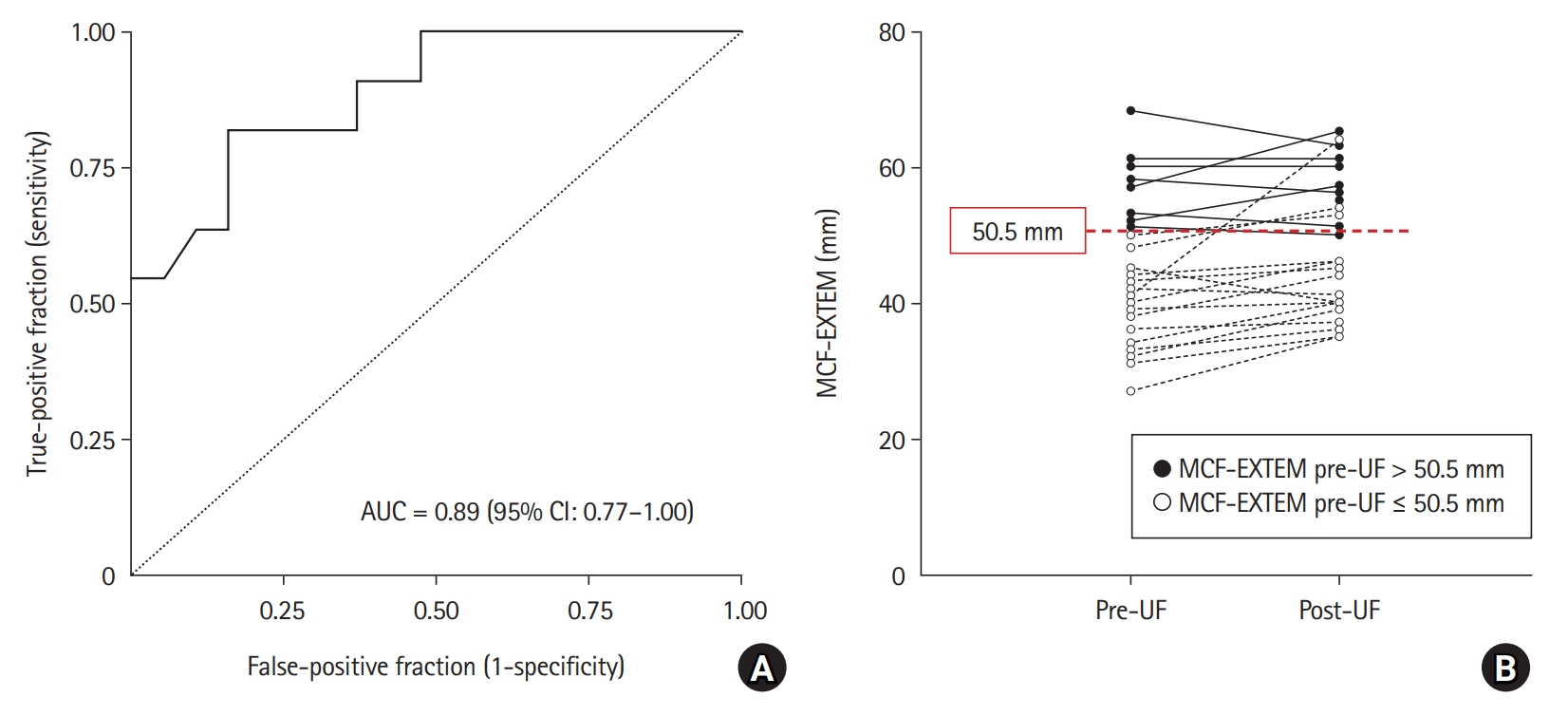 Effect of ultrafiltration on whole blood coagulation profile during cardiopulmonary bypass in cardiac surgery: a retrospective analysis
Effect of ultrafiltration on whole blood coagulation profile during cardiopulmonary bypass in cardiac surgery: a retrospective analysis
- Jaemoon Lee, Dong-Kyu Lee, Won-Kyoung Kwon, Sookyung Lee, Chung-Sik Oh, Klaus Görlinger, Tae-Yop Kim
-
Korean J Anesthesiol. 2024;77(2):236-245.
-
Clinical Research Article
January 30, 2024
|
-
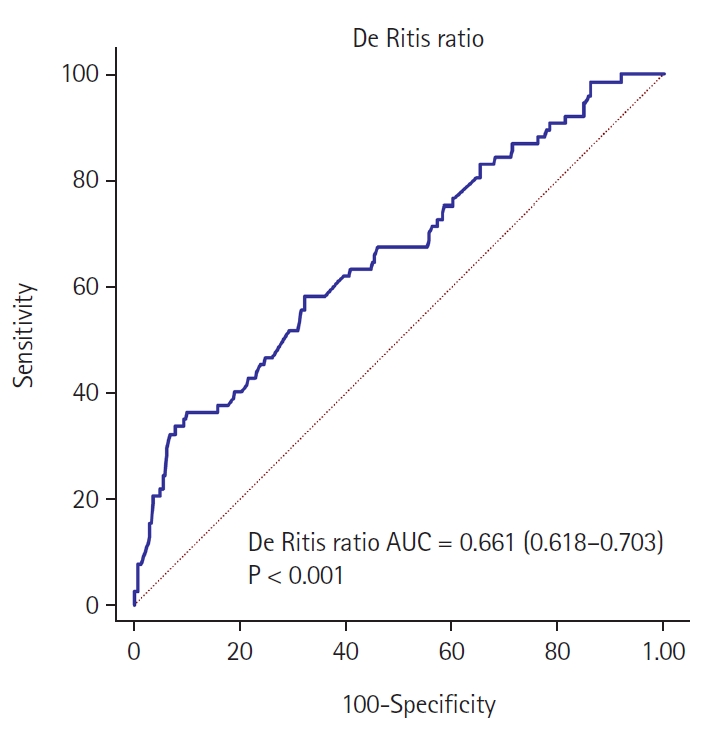 Association between De Ritis ratio and intraoperative blood transfusion in patients undergoing surgical clipping of unruptured intracranial aneurysms: a single center, retrospective, propensity score-matched study
Association between De Ritis ratio and intraoperative blood transfusion in patients undergoing surgical clipping of unruptured intracranial aneurysms: a single center, retrospective, propensity score-matched study
- Ji-Hoon Sim, Chan-Sik Kim, Seungil Ha, Hyunkook Kim, Yong-Seok Park, Joung Uk Kim
-
Korean J Anesthesiol. 2024;77(2):246-254.
-
Clinical Research Article
November 13, 2023
|
-
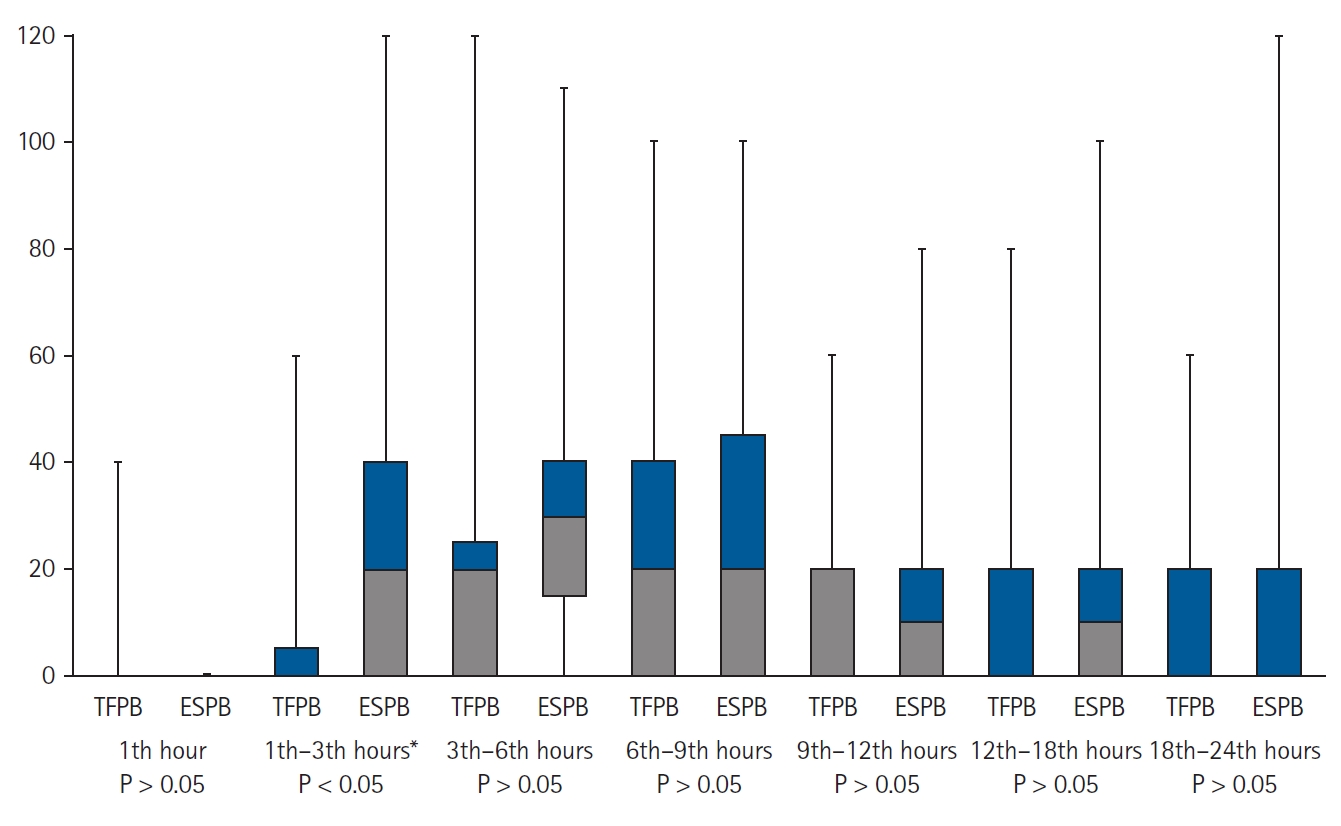 Comparison of the analgesic efficacy of the ultrasound-guided transversalis fascia plane block and erector spinae plane block in patients undergoing open inguinal hernia repair under spinal anesthesia
Comparison of the analgesic efficacy of the ultrasound-guided transversalis fascia plane block and erector spinae plane block in patients undergoing open inguinal hernia repair under spinal anesthesia
- Hale Kefeli Çelik, Serkan Tulgar, Ömer Faruk Bük, Kadem Koç, Murat Ünal, Caner Genç, Mustafa Süren
-
Korean J Anesthesiol. 2024;77(2):255-264.
-
Clinical Research Article
January 8, 2024
|
-
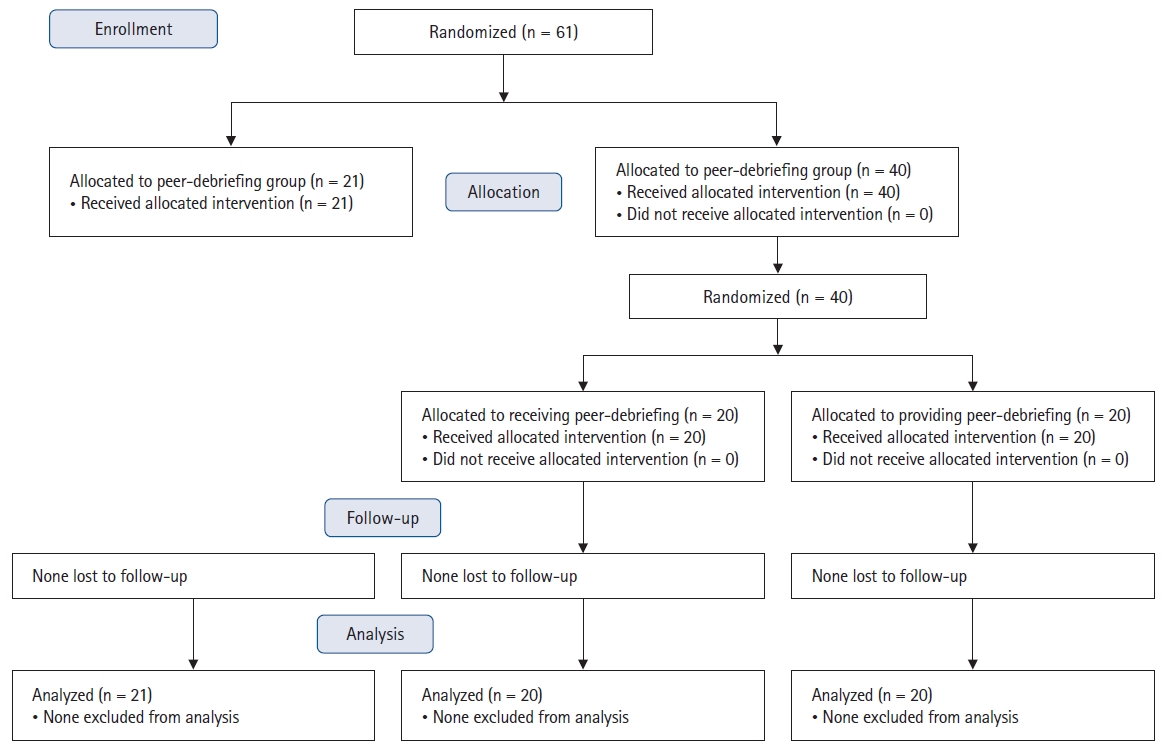 Learning with our peers: peer-led versus instructor-led debriefing for simulated crises, a randomized controlled trial
Learning with our peers: peer-led versus instructor-led debriefing for simulated crises, a randomized controlled trial
- Morgan Jaffrelot, Sylvain Boet, Yolande Floch, Nitan Garg, Daniel Dubois, Violaine Laparra, Lionel Touffet, M. Dylan Bould
-
Korean J Anesthesiol. 2024;77(2):265-272.
-
Experimental Research Article
March 29, 2024
|
-
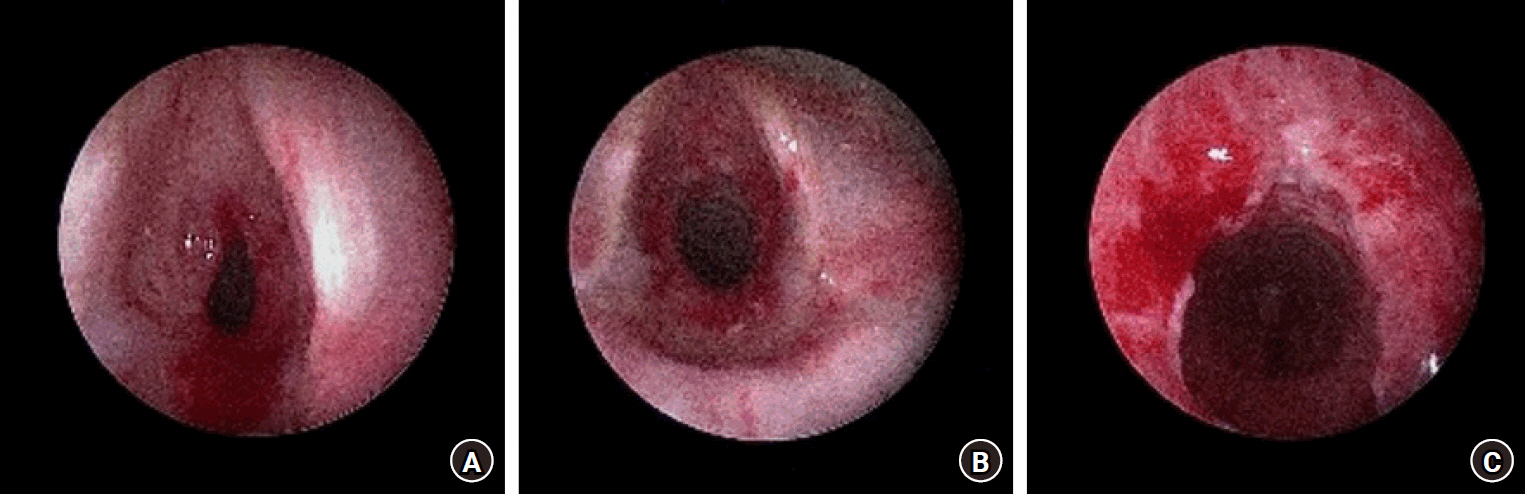 Use of oxygen reserve index during bronchoscopic balloon dilation for subglottic stenosis in a patient with left ventricular assist device implantation -a case report-
Use of oxygen reserve index during bronchoscopic balloon dilation for subglottic stenosis in a patient with left ventricular assist device implantation -a case report-
- Jimin Lee, Minwoo Chung, Eui-Suk Sung, Jung-Pil Yoon, Yeong Min Yoo, Jaesang Bae, Hee Young Kim
-
Korean J Anesthesiol. 2024;77(2):273-277.
-
Case Report
October 6, 2023
|
-
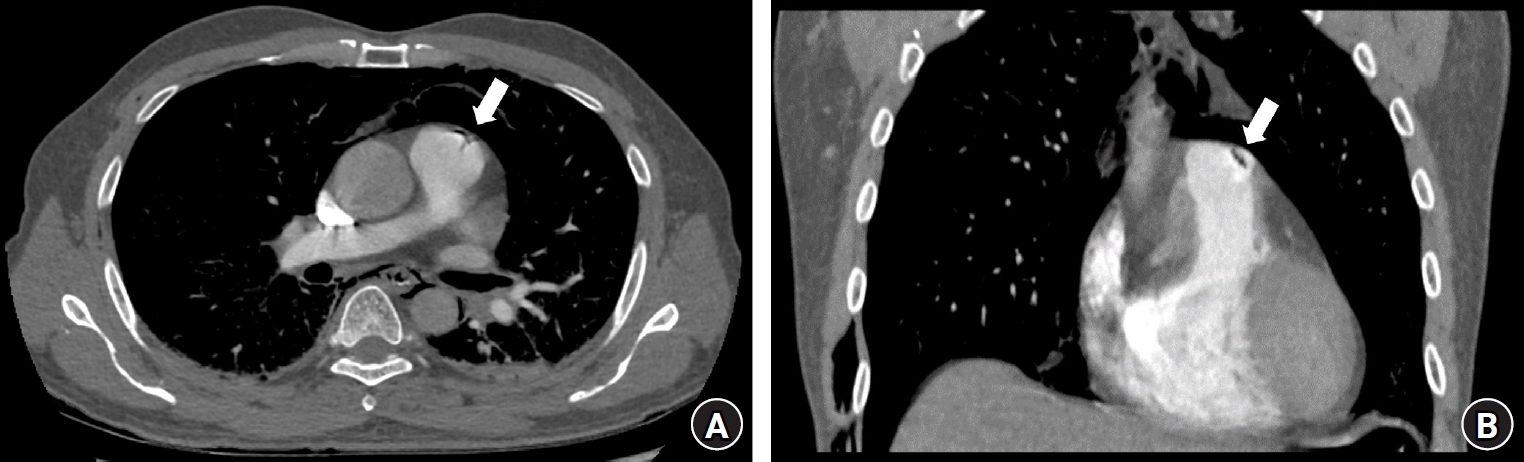 Venous air emboli during esophagoscopy confirmed by computed tomographic pulmonary angiography -a case report-
Venous air emboli during esophagoscopy confirmed by computed tomographic pulmonary angiography -a case report-
- Thadakorn Tantisarasart, Thara Tantichamnankul, Chanatthee Kitsiripant, Panjai Choochuen
-
Korean J Anesthesiol. 2024;77(2):278-281.
-
Case Report
November 29, 2023
|
-
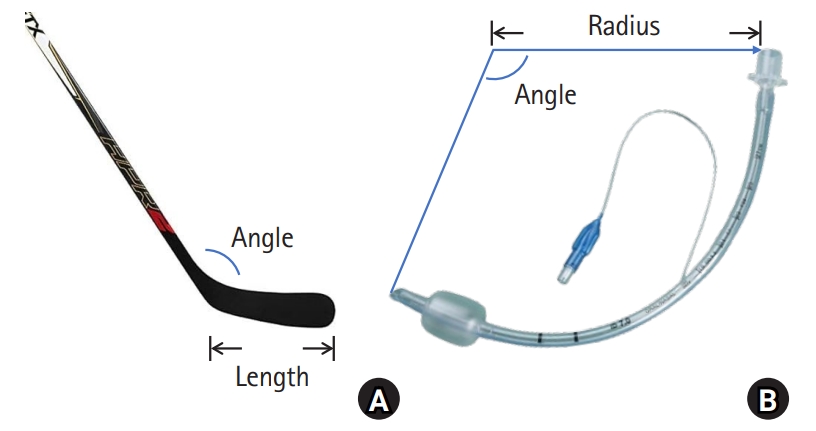 Comment on "Usefulness of C-curved stylet for intubation with the C-MAC® Miller videolaryngoscope in neonates and infants: a prospective randomized controlled trial"[commentary-article]
Comment on "Usefulness of C-curved stylet for intubation with the C-MAC® Miller videolaryngoscope in neonates and infants: a prospective randomized controlled trial"[commentary-article]
- Dong Ho Park, Jong Dal Chung, Chang Young Jeong, Hong-seuk Yang
-
Korean J Anesthesiol. 2024;77(2):282-283.
-
Letter to the Editor
January 26, 2024
|
-
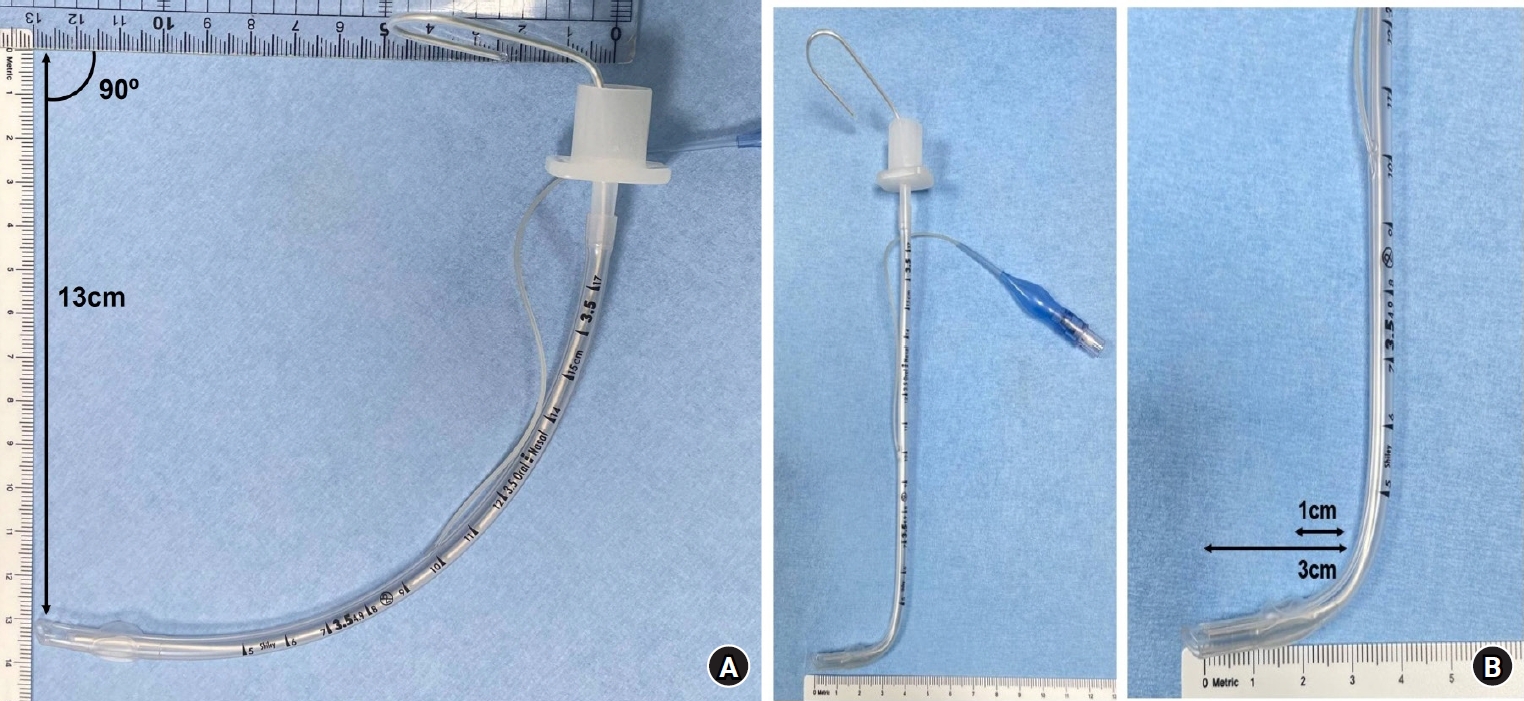 Response to "Comment on Usefulness of C-curved stylet for intubation with the C-MAC® Miller videolaryngoscope in neonates and infants: a prospective randomized controlled trial"
Response to "Comment on Usefulness of C-curved stylet for intubation with the C-MAC® Miller videolaryngoscope in neonates and infants: a prospective randomized controlled trial"
- Jung-Bin Park, Ji-Hyun Lee
-
Korean J Anesthesiol. 2024;77(2):283-284.
-
Letter to the Editor
January 26, 2024
|
-
Association of the perfusion index with postoperative acute kidney injury: a retrospective study
- Pyoyoon Kang, Jung-bin Park, Hyun-Kyu Yoon, Sang-Hwan Ji, Young-Eun Jang, Eun-Hee Kim, Ji-Hyun Lee, Hyung Chul Lee, Jin-Tae Kim, Hee-Soo Kim
-
Korean J Anesthesiol. 2024;77(2):285-285.
Corrects: Korean J Anesthesiol 2023 8; 76(4): 348
-
Corrigendum
March 29, 2024
|












")

















")












