Interfascial plane blocks have become popular in daily anesthesia practice in the field of acute and chronic pain management [1]. Owing to the use of ultrasound (US), novel plane blocks are increasingly being developed. To reduce controversy regarding the names and properties of these novel blocks, American Society of Regional Anesthesia and Pain Medicine (ASRA)-European Society of Regional Anaesthesia and Pain Therapy (ESRA) consensus published a nomenclature study [2]. Despite this, new descriptions of novel techniques continue to be defined. Kose et al. [3] has proposed that the deep supraspinatus muscle plane block (DSMPB), which involves the administration of local anesthetic (LA) into the plane between the supraspinatus muscles (SMs) and the posterior scapula, is a safer and easier novel technique. Recently, Teles et al. [4] called the DSMPB, a ŌĆ£new old techniqueŌĆØ since the block is basically an indirect anatomical landmark-guided suprascapular nerve block (SNB) verified by US. In contrast, Ciftci et al. [5] emphasized the different injection points used for the two blocks, namely, the needle is inserted approximately 2.5 cm away from the suprascapular notch for an SNB, while the insertion point for a DSMPB is 4 cm away and therefore likely to act under the principles of interfacial plane blocks. Given this controversy, we performed a cadaveric study to directly test whether the US-guided DSMPB and landmark-guided (US-verified) SNB would result in a similar anatomical area of coverage.
This study was performed after obtaining ethical approval from the Istanbul Medipol University Ethics and Research Committee (decision No. 715). One fresh male human cadaver was obtained by the Anatomy Department of Istanbul Medipol University. Since the study was approved by the ethics committee of our university and all rights of the cadaver belong to the anatomy department, no permissions were required for the use of the cadaver for our study. All injections were performed by two investigators with experience (at least 10 yearsŌĆÖ experience) administering US-guided fascial plane blocks. The cadaver was placed in the prone position and the cadaverŌĆÖs back, especially around the scapula, was fully inspected for anomalies. On the right side of the cadaverŌĆÖs back, US-guided (B-Braun, XperiusTM, B.Braun Melsungen AG, Germany) DSMPB was performed with a multifrequency 11ŌĆō12 MHz linear probe covered with a protective plastic sheath. The probe was placed at the base of the spinae scapula in the transverse plane and was slowly moved cranially to visualize the trapezius and SM on the medial side of the scapula. A 22 gauge (G), 100 mm needle (Stimuplex┬« Ultra 360, B-Braun, B.ŌĆēBraun Melsungen AG, Germany) was punctured medially to laterally using the in-plane technique. The needle was inserted below the SM and in contact with the supraspinous fossa. Twenty ml of 0.25% methylene blue dye was injected here. On the left side of the cadaverŌĆÖs back, a landmark-guided SNB was performed. The scapula was separated into quadrants using a vertical line that passed along the length of the scapular spine. The point in the upper outer quadrant (2.5 cm lateral to the vertical line) was targeted. In order to verify the injection point, an US probe was placed on the targeted point over the scapular spine. After visualizing the suprascapular notch, a 22 G, 100 mm needle (Stimuplex┬« Ultra 360, B-Braun, B.ŌĆēBraun Melsungen AG, Germany) was inserted using the in-plane technique. A total of 20 ml of 0.25% methylene blue dye was injected at this location.
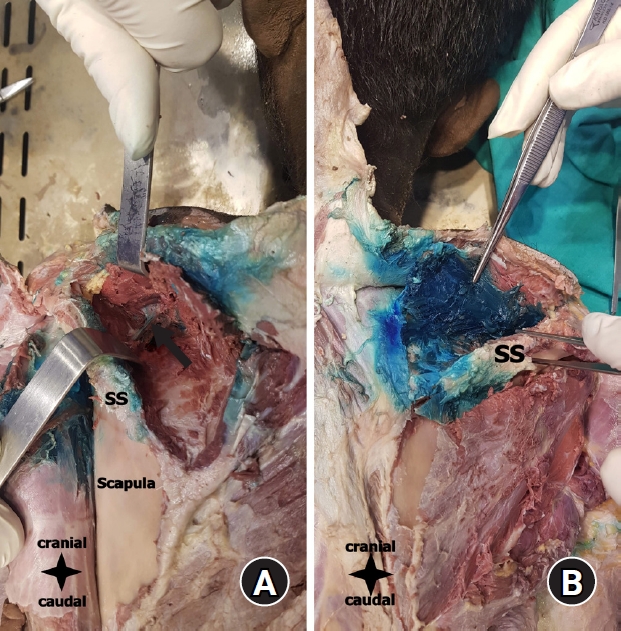
Anatomic dissections were performed by the same anatomists using a standardized method 20 min after the procedures. A midline skin incision was made from the protuberantia occipitalis externa to the coccyx. A second incision was made from the acromion through the spinae scapula. After the incisions were combined, the skin was retracted laterally to visualize the posterior thoracic wall and scapula. The trapezius muscle was reflected from the spinous processes and spinae scapula, after which the scapula, supraspinatus muscle, and infraspinatus muscle were visualized. The supraspinatus and infraspinatus muscles were dissected from the medial margin of the scapula and spinae scapula. On the left side (SNB), the dye had spread to the supraspinous fossa, with minimal dye spread around the shoulder joint capsule from the view of the quadrangular space. Methylene blue was also observed around the suprascapular nerve (Fig. 1A). On the right side (DSMPB), the dye had spread densely in the supraspinous fossa region (Fig. 1B). Methylene blue was observed on both the anterior and posterior sides of the SM. There was also dye visualized on the spinae scapula, but no methylene blue could be seen in the infraspinous fossa.
We agree with Teles et al. [4] on the point that, given the abundance of novel nerve block approaches, significant heterogeneity exists in the nomenclature. Recently, an ASRA-ESRA Delphi consensus study was conducted to standardize the nomenclature and anatomical descriptions of paraspinal, chest wall, and abdominal wall blocks [2]. However, our findings suggest that it would be incorrect to describe DSMPB as a reinterpretation of the classical technique. Although the SNB and DSMPB covered some common areas over the scapula, the DSMPB provided a denser spread of dye in the supraspinous fossa than the SNB, while the SNB covered a larger area over both the supraspinous and infraspinous fossa. Our results suggest that SNBs may be used for pain control after major surgeries involving the shoulder joint or for chronic pain management, while DSMPBs may be better suited for chronic pain treatment or management after minor shoulder surgeries.